

Cardiac arrest as a reportable condition: a cohort study of the first 6 years of the Norwegian out-of-hospital cardiac arrest registry
- PMID: 32641339
- PMCID: PMC7348469
- DOI: 10.1136/bmjopen-2020-038133
Cardiac arrest as a reportable condition: a cohort study of the first 6 years of the Norwegian out-of-hospital cardiac arrest registry
Abstract
Objectives: The Norwegian Cardiac Arrest Registry (NorCAR) was established in 2013 when cardiac arrest became a mandatory reportable condition. The aim of this cohort study is to describe how the world's first mandatory, population-based cardiac arrest registry evolved during its first 6 years.
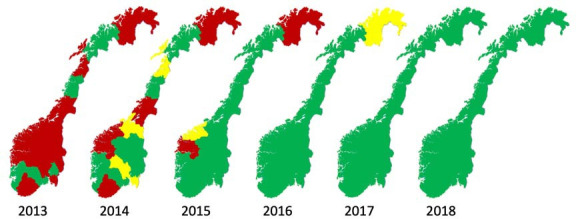
Setting: Norway has a total population of 5.3 million inhabitants with a population density that varies considerably. All residents are assigned a unique identifier number, giving nationally approved registries access to information about all births and deaths in the country. Data in the registry are entered by data processors; public employees with close links to the emergency medical services. All data processors undergo a standardised training and meet for yearly retraining and updates.
Participants: All events of cardiac arrest where bystanders or healthcare professionals have started cardiopulmonary resuscitation or performed defibrillation are included into the NorCAR.
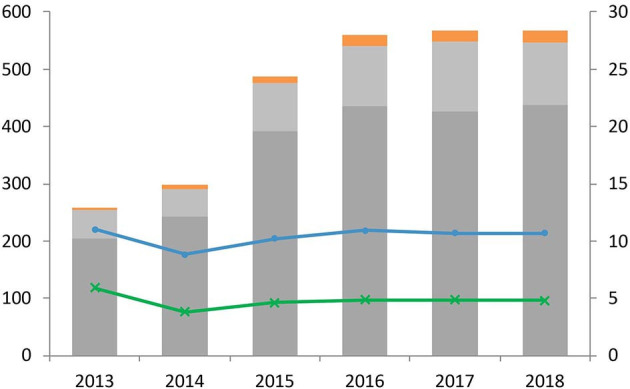
Primary and secondary outcome measures: Since the establishment of the registry, the number of reporting health trusts, the number of reported events and the corresponding population at risk were followed year by year. Outcome is measured as changes in inclusion rate, incidence per 100 000 inhabitants and survival to 30 days after cardiac arrest.
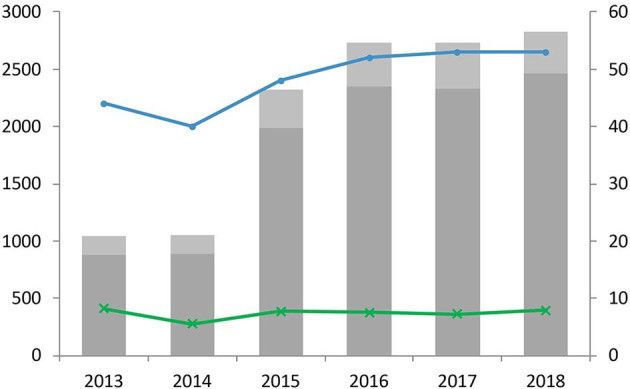
Results: In total, 14 849 cases were registered over 6 years, between 2013 and 2018. The number of health trusts reporting rose steadily from 2013. Within 3 years, all trusts reported to the registry with an increasing number of events reported; going from 1101 to 3400 per year. The prevalence of bystander cardiopulmonary resuscitation increased slightly, but the population incidence of survival did not change.
Conclusion: Declaring cardiac arrest as a reportable condition and close follow-up of all reporting areas is essential when building a national registry.
Keywords: cardiac arrest; cardiology; epidemiology; registry; reporting.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: There are no competing interests to report for the submitted work. TMO reports grants from Zoll Foundation and grants from Laerdal foundation, outside the submitted work. TWL reports paid and unpaid consultant work for Lærdal Medical and the Norwegian Air Ambulance Foundation outside the submitted work.
Figures
References
-
- Meaney PA, Bobrow BJ, Mancini ME, et al. . Cardiopulmonary resuscitation quality: [corrected] improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association. Circulation 2013;128:417–35. 10.1161/CIR.0b013e31829d8654 - DOI - PubMed
-
- Global Resuscitation Alliance Secondary global resuscitation alliance 2017. Available: https://www.globalresuscitationalliance.org [Accessed 21 Apr 2020].
MeSH terms
LinkOut - more resources
Full Text Sources
Medical