

Impact of the herpes zoster vaccination programme on hospitalised and general practice consulted herpes zoster in the 5 years after its introduction in England: a population-based study
- PMID: 32641364
- PMCID: PMC7342826
- DOI: 10.1136/bmjopen-2020-037458
Impact of the herpes zoster vaccination programme on hospitalised and general practice consulted herpes zoster in the 5 years after its introduction in England: a population-based study
Abstract
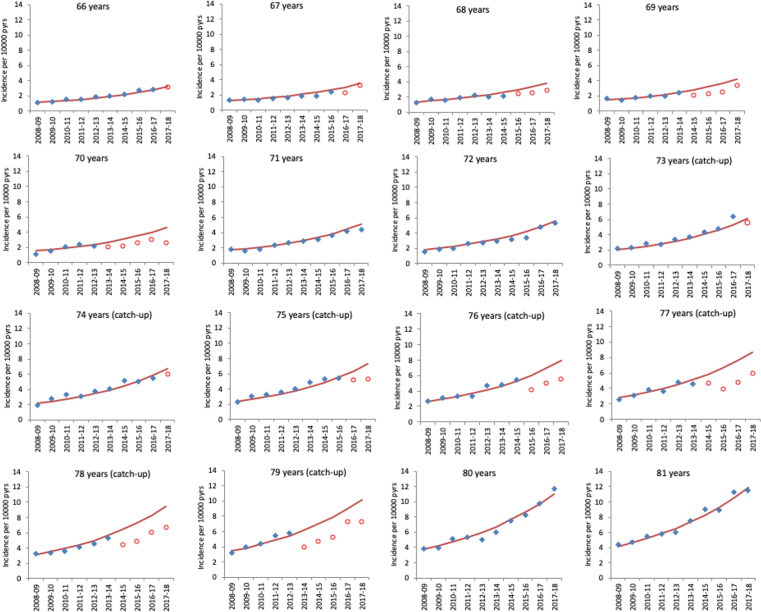
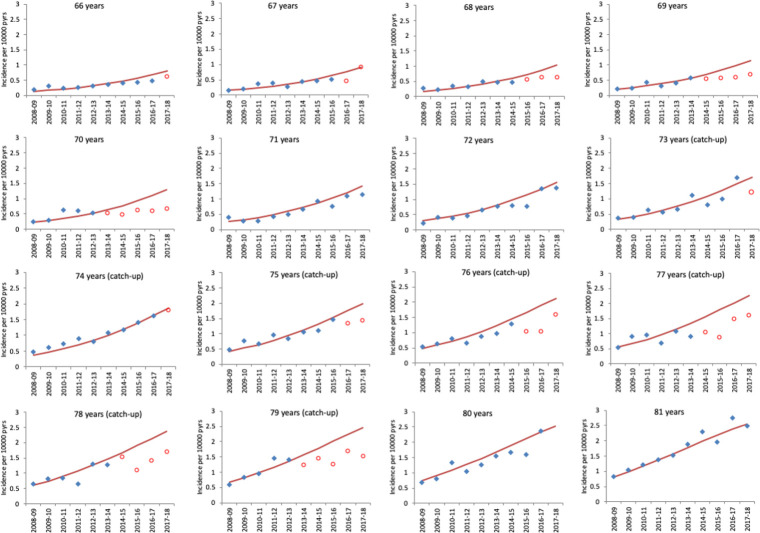
Objectives: To assess the impact of herpes zoster vaccination in the 5 years after introduction for 70- to 79-year-olds in England in September 2013.
Design: Population based ecological impact assessment.
Setting: Hospitals covering the whole English population for the period 2008 to 2018 and 293 general practices (GP) for the period 2005 to 2018, in England.
Participants: Over the period the population contributed 117·5 million person-years for hospitalisation events and 6.96 million person-years for GP events in individuals aged 60 to 89.
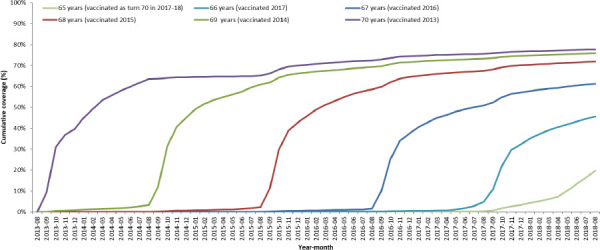
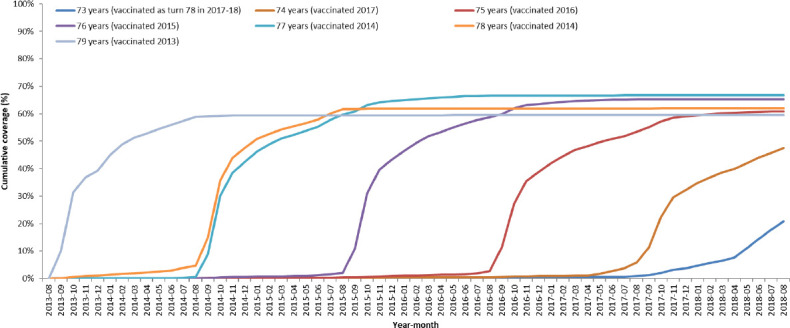
Interventions: Live attenuated herpes zoster vaccination (Zostavax), first used on 1st September 2013, in 70- and 79-year-olds with continued use in new 70 year-olds and with a staged catch-up of those aged 71 to 78 years in 2013.
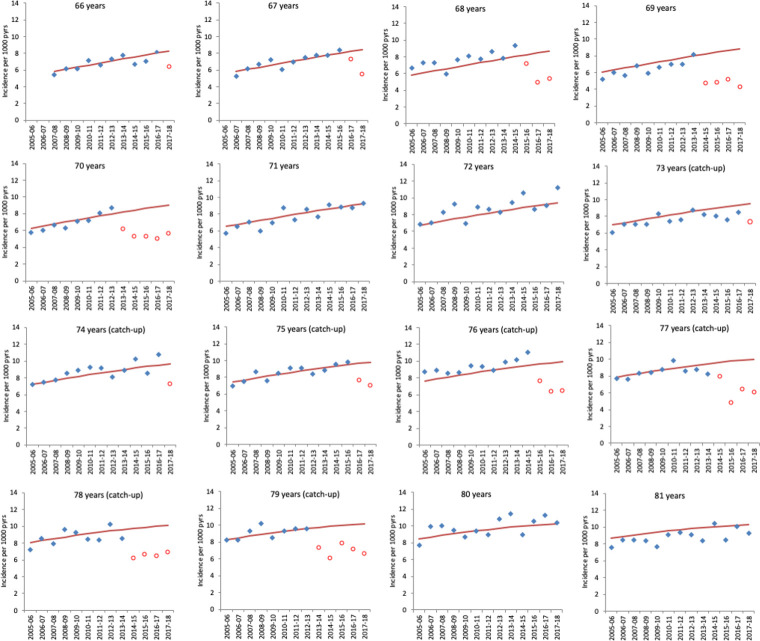
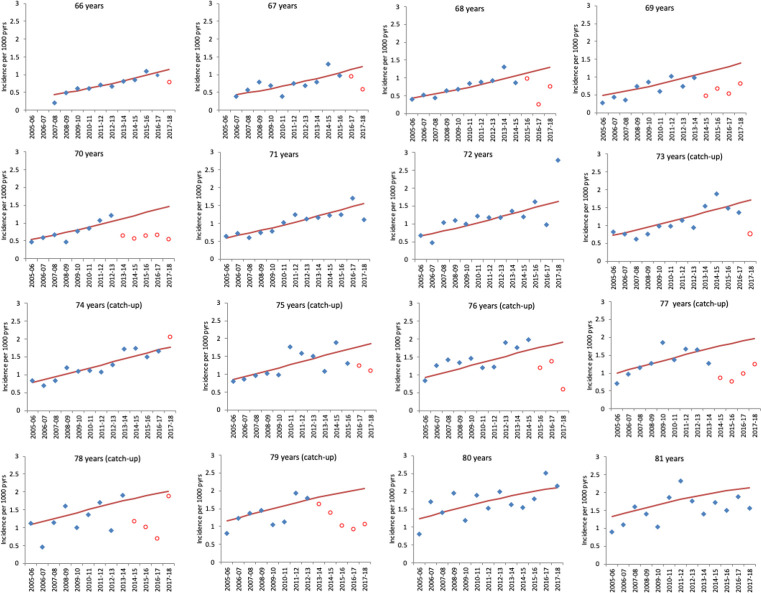
Outcome measures: Herpes zoster and postherpetic neuralgia (PHN) consultation and hospitalisation rates in age-cohorts according to vaccine eligibility. Incidence rate ratios in age-cohorts eligible for vaccination compared with those non-eligible were calculated by Poisson regression. This was used to estimate prevented cases and, along with vaccine coverage, to estimate vaccine effectiveness.
Results: Large and prolonged reductions in herpes zoster and PHN consultations and hospitalisations were observed in the 5 years post-implementation. For example, in 79 year-olds first eligible in 2013, the incidence rate ratio for consultations 5 years later was 0·65 (95% CI: 0·52 to 0·81). Over the whole period an estimated 40 500 fewer zoster consultations and 1840 fewer zoster hospitalisations occurred because of the vaccination programme. These reductions were consistent with effectiveness in the routine cohorts (vaccinated aged 70) of between 37% (for hospitalised zoster) and 75% (for PHN consultations) and, in catch up cohorts (vaccinated aged 78 to 79) of between 49% (for hospitalised PHN) and 66% (for PHN consultations).
Conclusion: Given the clear and sustained impact of herpes zoster vaccination over the 5-year period since introduction, optimising vaccination coverage is important to attain maximum benefit.
Keywords: epidemiology; health economics; paediatric infectious disease & immunisation; public health.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: SdeL has received University funding for studies of post vaccination adverse events of interest from GSK, and for attitudes to vaccination from Seqirus; and has been a member of Seqirus and Sanofi advisory boards. Public Health England, National Infection Service, Immunisation and Countermeasures Division has provided vaccine manufacturers with post-marketing surveillance reports, which the Marketing Authorisation Holders are required to submit to the UK licensing authority in compliance with their Risk Management Strategy. A cost recovery charge is made for these reports.
Figures
References
-
- Joint Committee on Vaccination and Immunisation Statement on varicella and herpes zoster vaccines. Available: http://webarchive.nationalarchives.gov.uk/20120907090205/http://www.dh.g...
-
- Public Health England Immunisation against infectious disease, the greenbook; chapter 28a shingles (herpes zoster). Available: https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical