

Transcriptional Changes in Kidney Allografts with Histology of Antibody-Mediated Rejection without Anti-HLA Donor-Specific Antibodies
- PMID: 32641395
- PMCID: PMC7461663
- DOI: 10.1681/ASN.2020030306
Transcriptional Changes in Kidney Allografts with Histology of Antibody-Mediated Rejection without Anti-HLA Donor-Specific Antibodies
Abstract
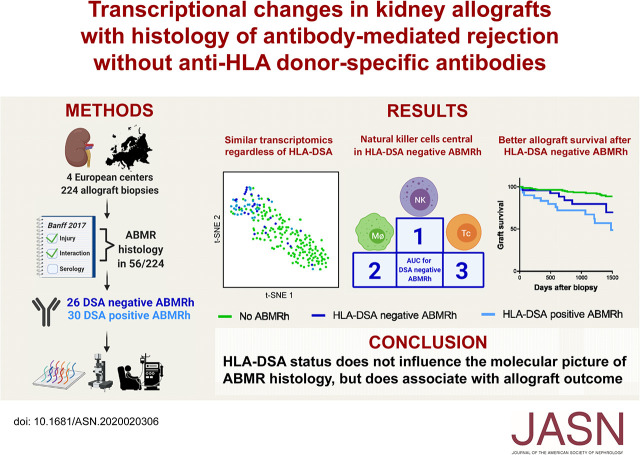
Background: Circulating donor-specific anti-HLA antibodies (HLA-DSAs) are often absent in serum of kidney allograft recipients whose biopsy specimens demonstrate histology of antibody-mediated rejection (ABMR). It is unclear whether cases involving ABMR histology without detectable HLA-DSAs represent a distinct clinical and molecular phenotype.
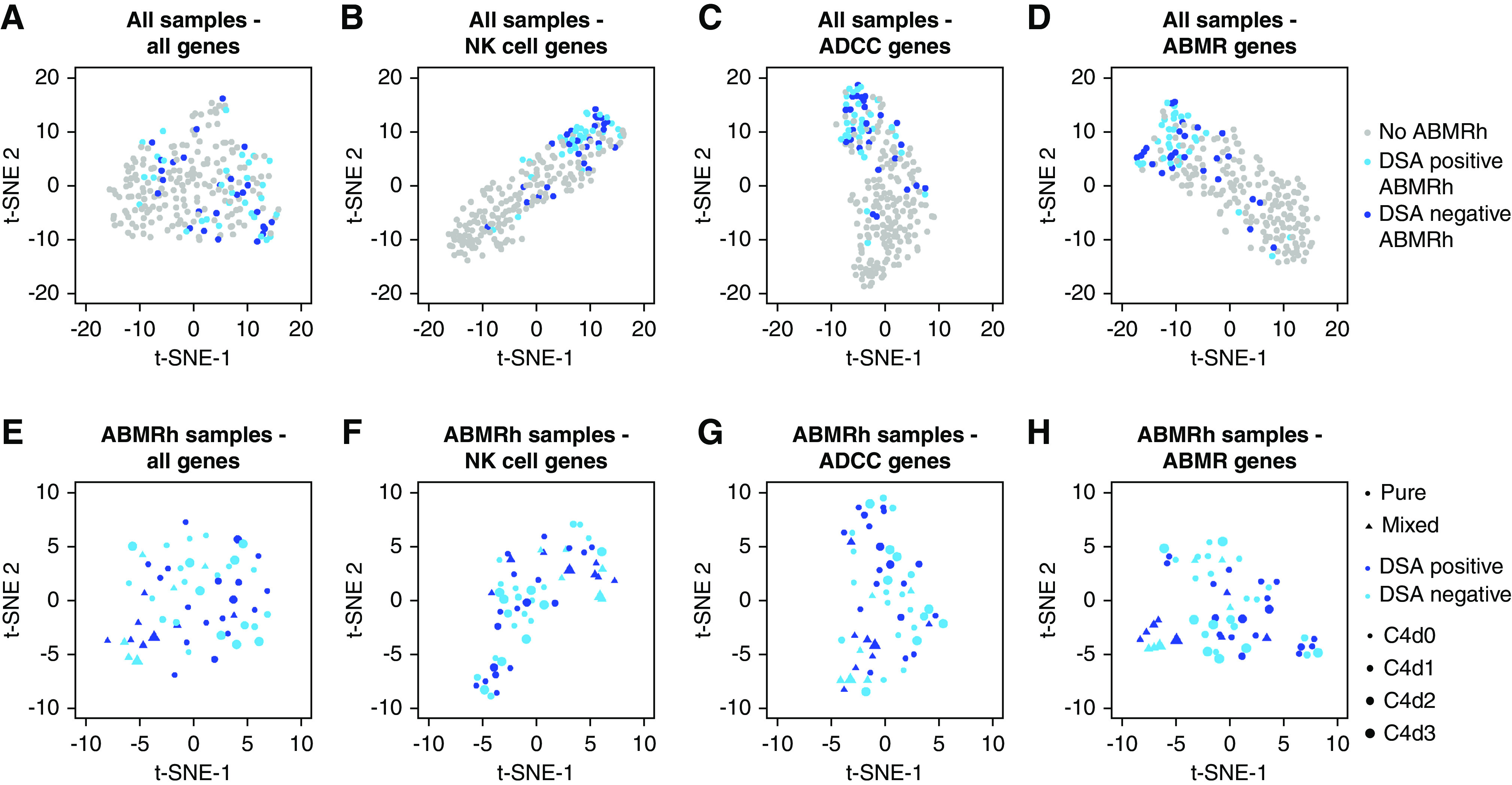
Methods: In this multicenter cohort study, we integrated allograft microarray analysis with extensive clinical and histologic phenotyping from 224 kidney transplant recipients between 2011 and 2017. We used the term ABMR histology for biopsy specimens that fulfill the first two Banff 2017 criteria for ABMR, irrespective of HLA-DSA status.
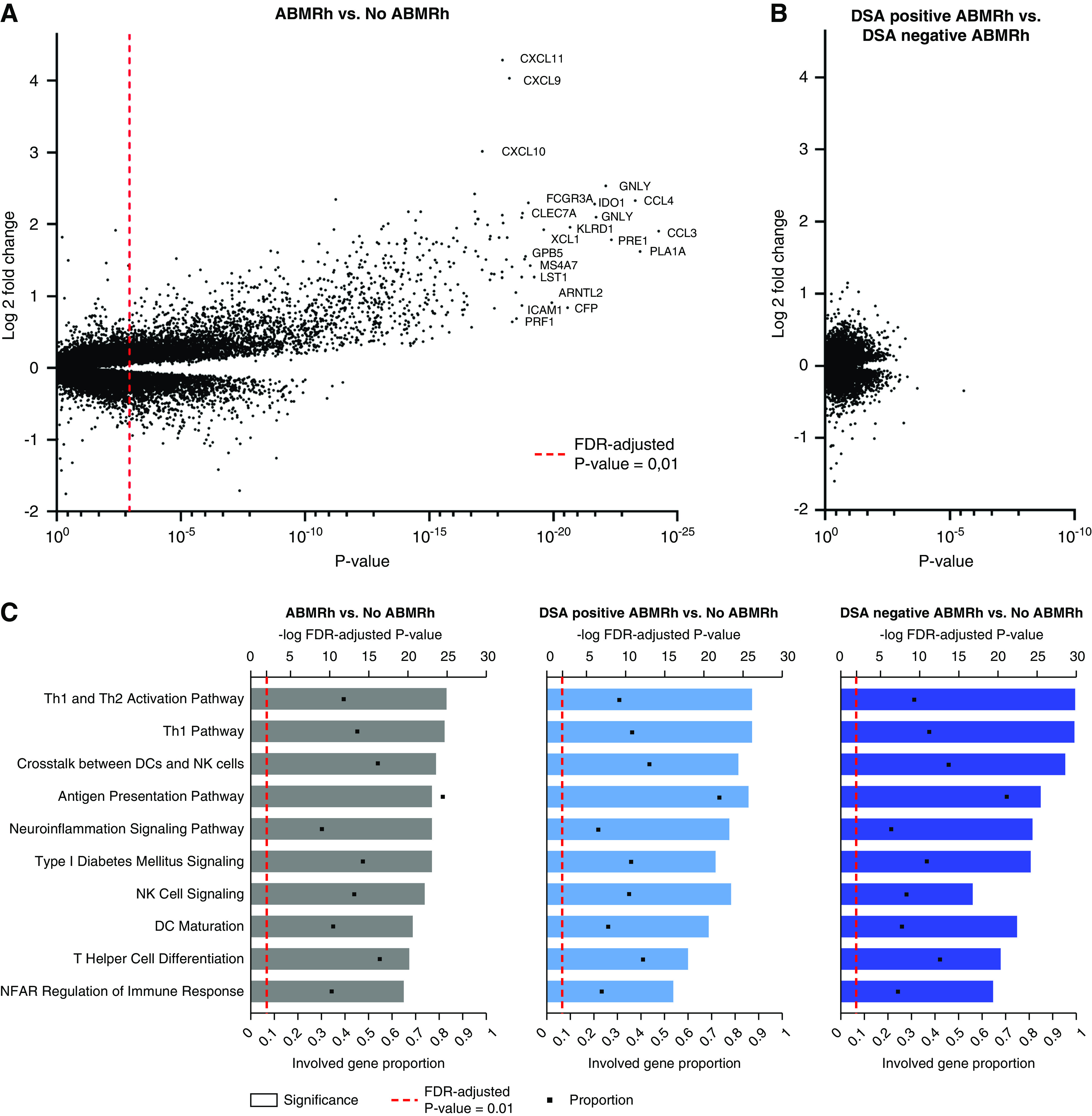
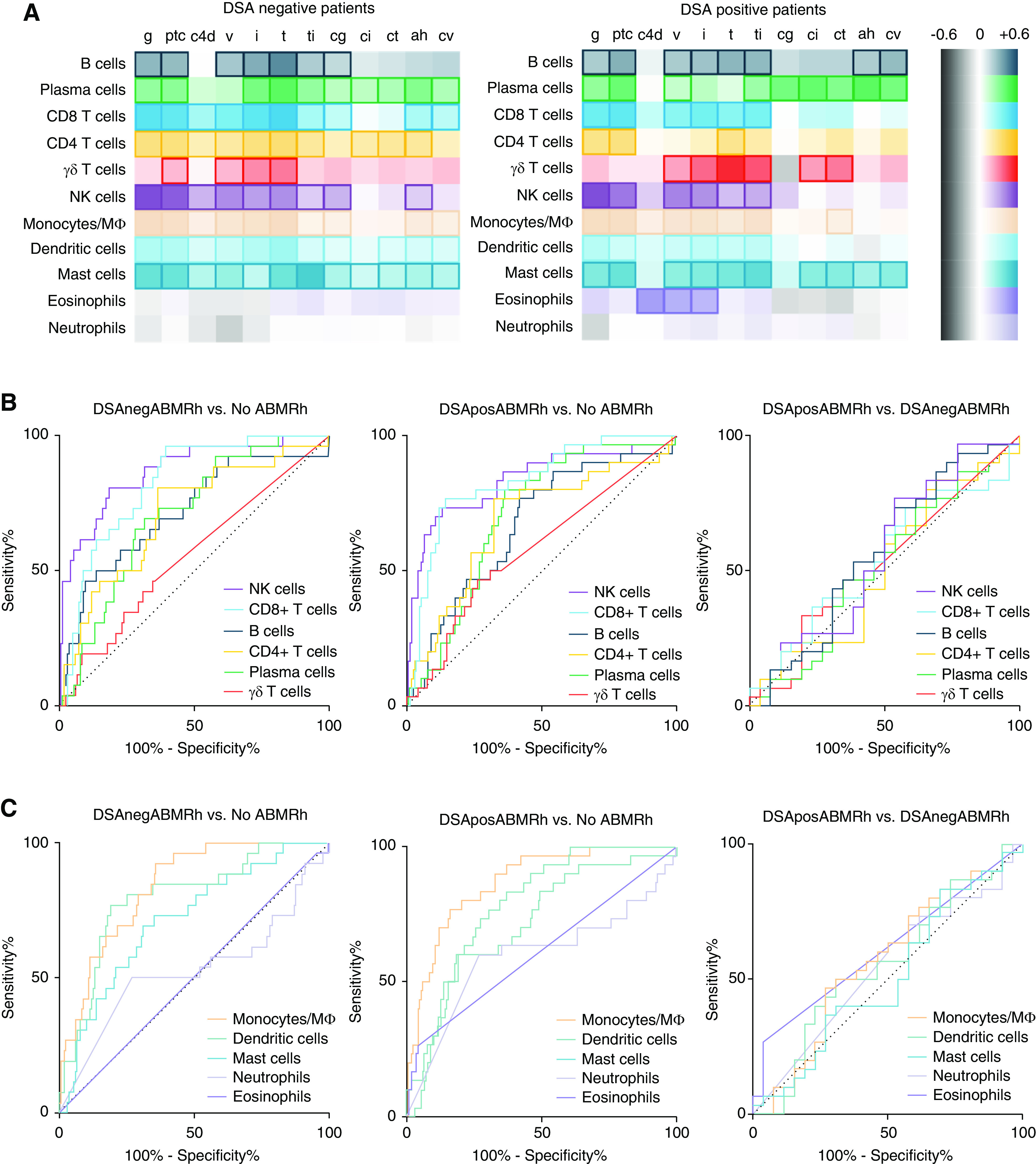
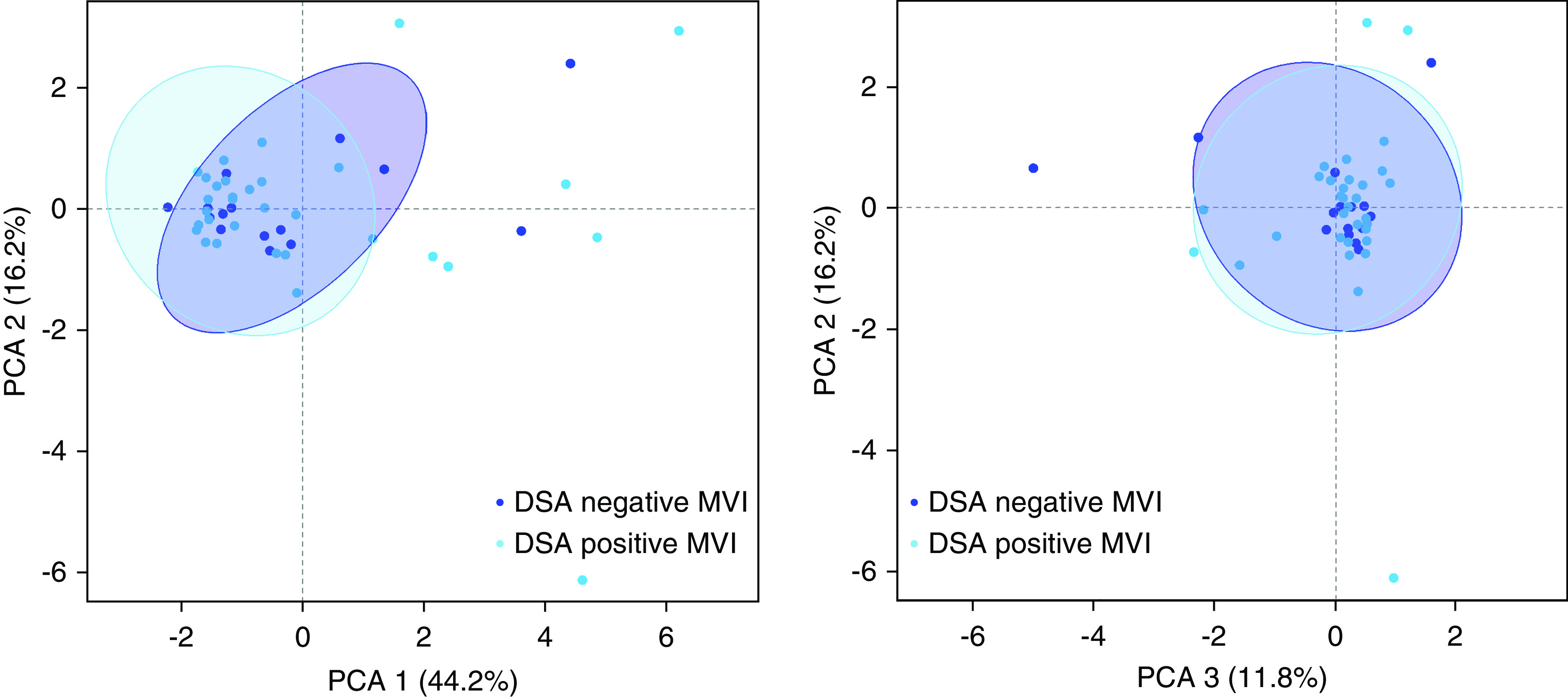
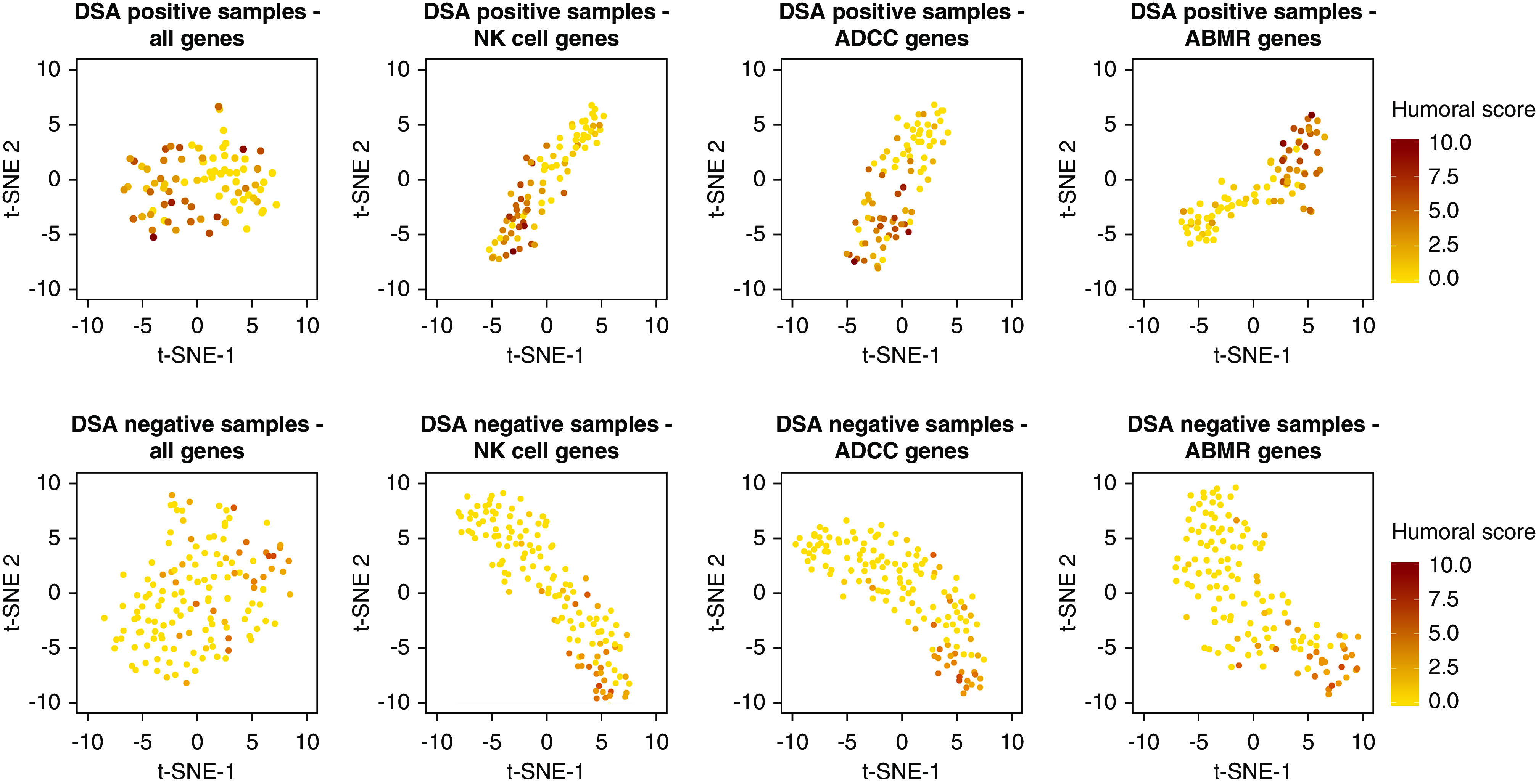
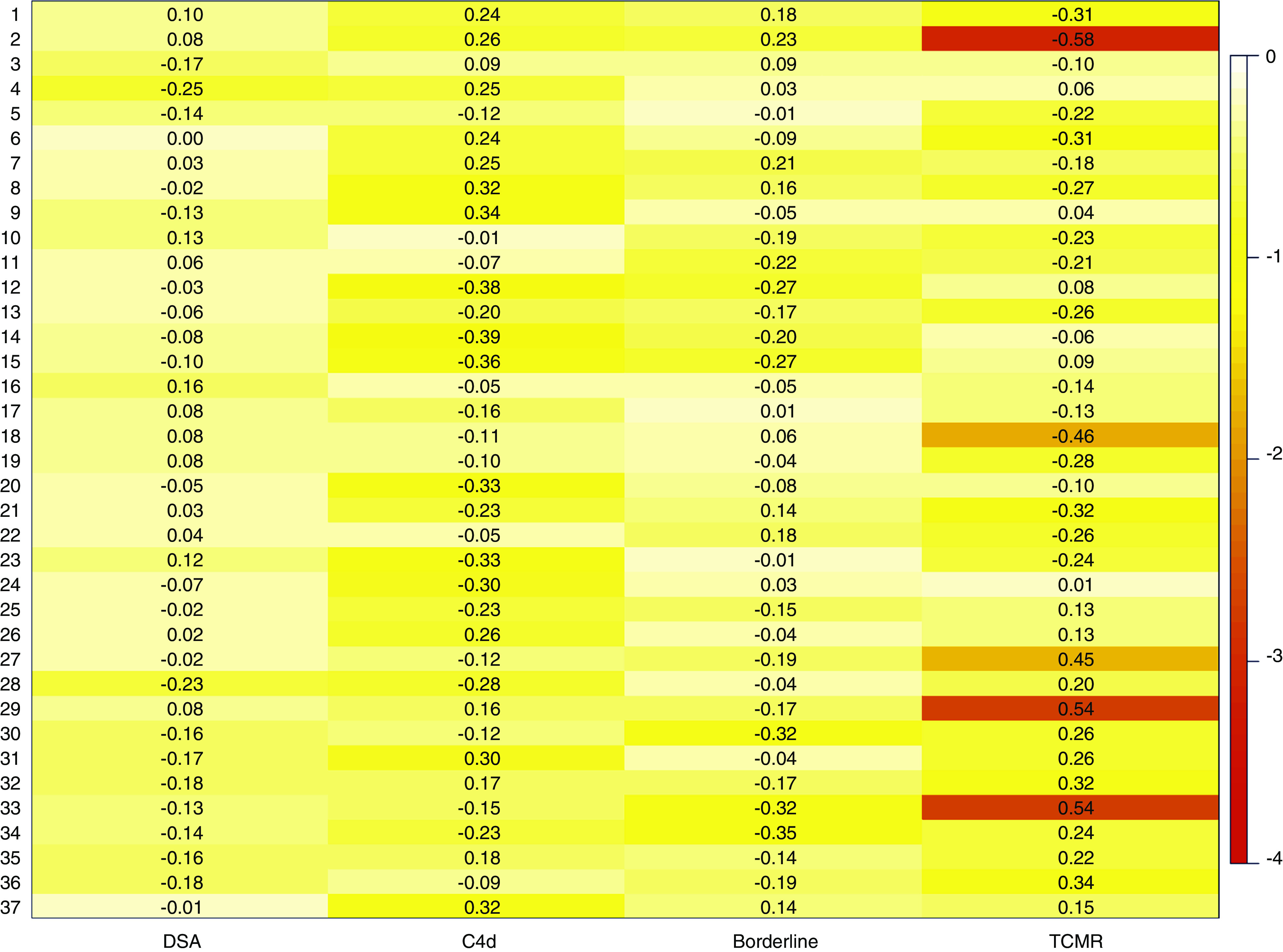
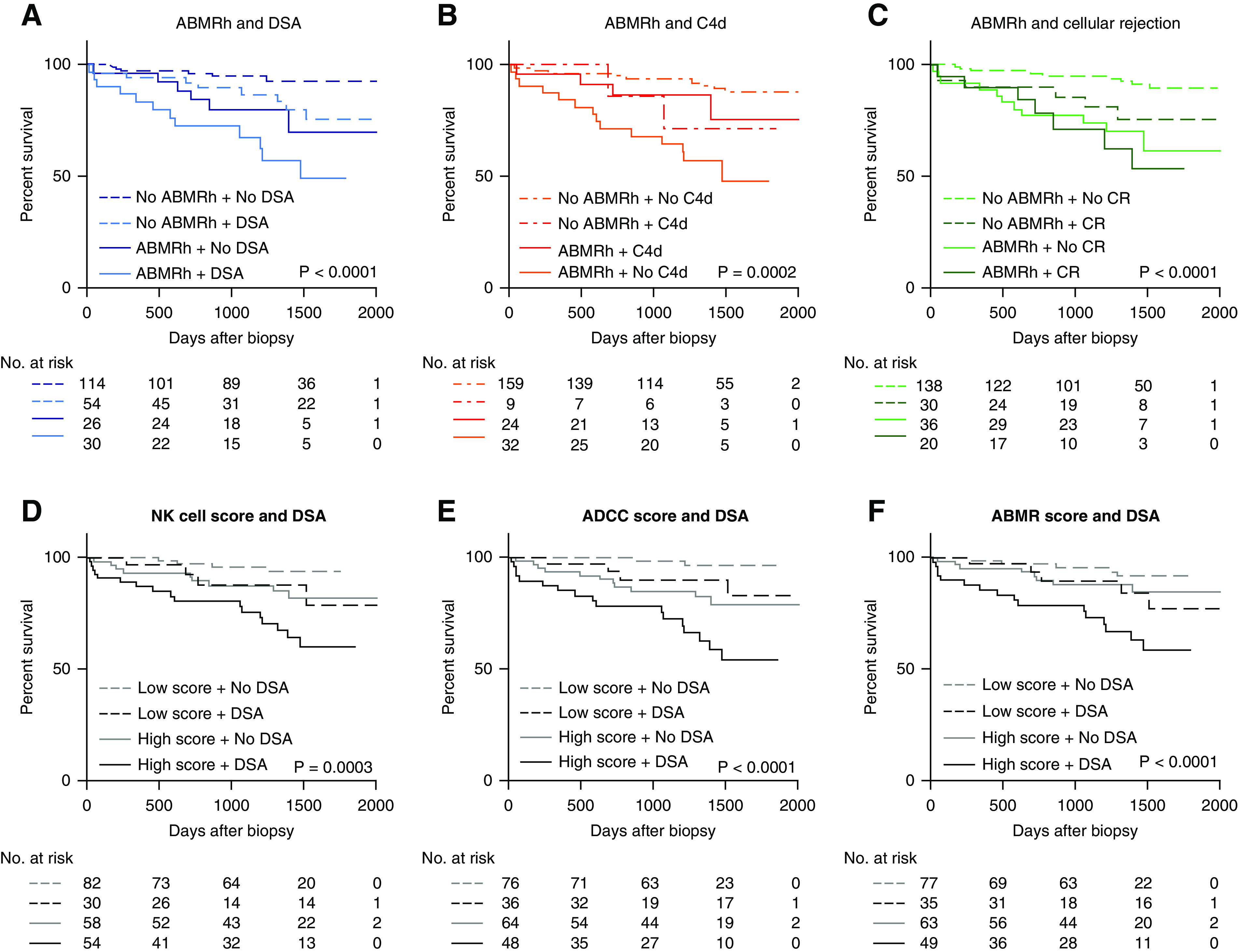
Results: Of 224 biopsy specimens, 56 had ABMR histology; 26 of these (46.4%) lacked detectable serum HLA-DSAs. Biopsy specimens with ABMR histology showed overexpression of transcripts mostly related to IFNγ-induced pathways and activation of natural killer cells and endothelial cells. HLA-DSA-positive and HLA-DSA-negative biopsy specimens with ABMR histology displayed similar upregulation of pathways and enrichment of infiltrating leukocytes. Transcriptional heterogeneity observed in biopsy specimens with ABMR histology was not associated with HLA-DSA status but was caused by concomitant T cell-mediated rejection. Compared with cases lacking ABMR histology, those with ABMR histology and HLA-DSA had higher allograft failure risk (hazard ratio [HR], 7.24; 95% confidence interval [95% CI], 3.04 to 17.20) than cases without HLA-DSA (HR, 2.33; 95% CI, 0.85 to 6.33), despite the absence of transcriptional differences.
Conclusions: ABMR histology corresponds to a robust intragraft transcriptional signature, irrespective of HLA-DSA status. Outcome after ABMR histology is not solely determined by the histomolecular presentation but is predicted by the underlying etiologic factor. It is important to consider this heterogeneity in further research and in treatment decisions for patients with ABMR histology.
Keywords: antibody-mediated rejection; donor-specific antibodies; kidney transplantation; natural killer cells; transcriptomics.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Coemans M, Süsal C, Döhler B, Anglicheau D, Giral M, Bestard O, et al.: Analyses of the short- and long-term graft survival after kidney transplantation in Europe between 1986 and 2015. Kidney Int 94: 964–973, 2018. - PubMed
-
- Lamb KE, Lodhi S, Meier-Kriesche HU: Long-term renal allograft survival in the United States: A critical reappraisal. Am J Transplant 11: 450–462, 2011. - PubMed
-
- Halloran PF: Immunosuppressive drugs for kidney transplantation. N Engl J Med 351: 2715–2729, 2004. - PubMed
-
- Naesens M, Kuypers DRJ, De Vusser K, Evenepoel P, Claes K, Bammens B, et al.: The histology of kidney transplant failure: a long-term follow-up study. Transplantation 98: 427–435, 2014. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
