

Cost-effectiveness of surgery for drug-resistant temporal lobe epilepsy in the US
- PMID: 32641528
- PMCID: PMC7538217
- DOI: 10.1212/WNL.0000000000010185
Cost-effectiveness of surgery for drug-resistant temporal lobe epilepsy in the US
Abstract
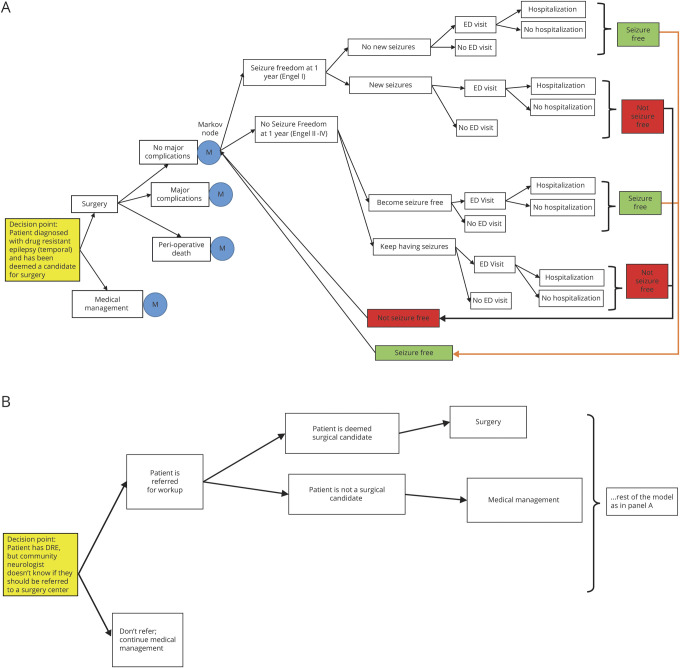
Objective: Surgery is an effective but costly treatment for many patients with drug-resistant temporal lobe epilepsy (DR-TLE). We aim to evaluate whether, in the United States, surgery is cost-effective compared to medical management for patients deemed surgical candidates and whether surgical evaluation is cost-effective for patients with DR-TLE in general.
Methods: We use a semi-Markov model to assess the cost-effectiveness of surgery and surgical evaluation over a lifetime horizon. We use second-order Monte Carlo simulations to conduct probabilistic sensitivity analyses to estimate variation in model output. We adopt both health care and societal perspectives, including direct health care costs (e.g., surgery, antiepileptic drugs) and indirect costs (e.g., lost earnings by patients and care providers.) We compare the incremental cost-effectiveness ratio to societal willingness to pay (∼$100,000 per quality-adjusted life-year [QALY]) to determine whether surgery is cost-effective.
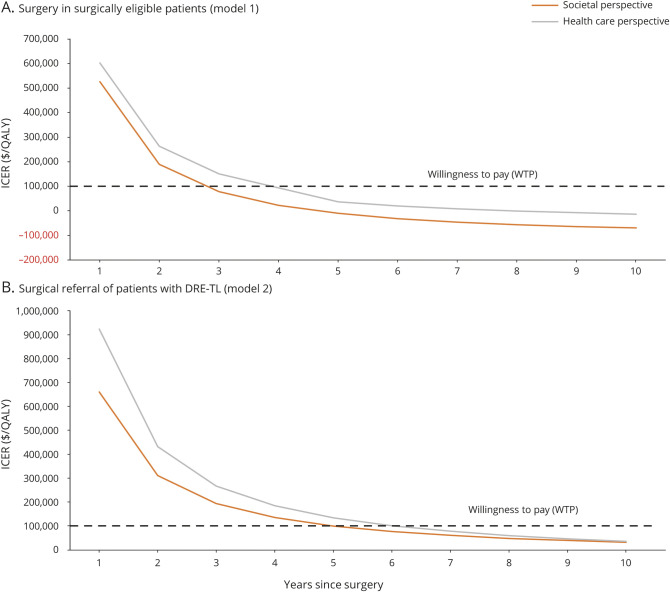
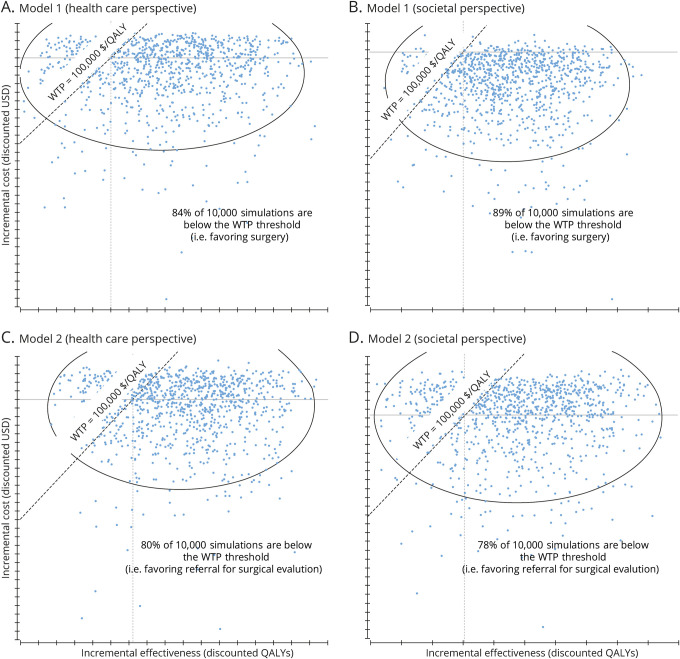
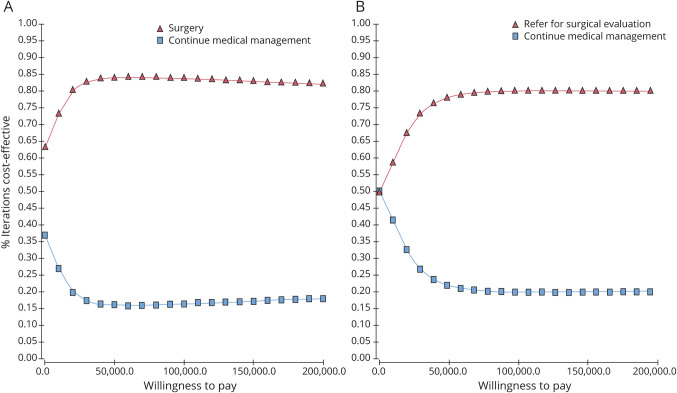
Results: Epilepsy surgery is cost-effective compared to medical management in surgically eligible patients by virtue of being cost-saving ($328,000 vs $423,000) and more effective (16.6 vs 13.6 QALY) than medical management in the long run. Surgical evaluation is cost-effective in patients with DR-TLE even if the probability of being deemed a surgical candidate is only 5%. From a societal perspective, surgery becomes cost-effective within 3 years, and 89% of simulations favor surgery over the lifetime horizon.
Conclusion: For surgically eligible patients with DR-TLE, surgery is cost-effective. For patients with DR-TLE in general, referral for surgical evaluation (and possible subsequent surgery) is cost-effective. Patients with DR-TLE should be referred for surgical evaluation without hesitation on cost-effectiveness grounds.
© 2020 American Academy of Neurology.
Figures
Comment in
-
Epilepsy surgery: Expensive, but worth the "price" of admission.Neurology. 2020 Sep 8;95(10):417-418. doi: 10.1212/WNL.0000000000010208. Epub 2020 Jul 8. Neurology. 2020. PMID: 32641524 No abstract available.
-
Dollars and Sense: Cost-Effectiveness of Epilepsy Surgery.Epilepsy Curr. 2021 Feb 22;21(3):171-172. doi: 10.1177/1535759721995191. eCollection 2021 May-Jun. Epilepsy Curr. 2021. PMID: 34867096 Free PMC article. No abstract available.
References
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med 2001;345:311–318. - PubMed
-
- Engel J Jr, Wiebe S, French J, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Epilepsia 2003;44:741–751. - PubMed
-
- Choi H, Sell RL, Lenert L, et al. Epilepsy surgery for pharmacoresistant temporal lobe epilepsy: a decision analysis. JAMA 2008;300:2497–2505. - PubMed
-
- Langfitt J, Holloway R, McDermott M, et al. Health care costs decline after successful epilepsy surgery. Neurology 2007;68:1290–1298. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources