

Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital
- PMID: 32641730
- PMCID: PMC7343863
- DOI: 10.1038/s41467-020-17318-x
Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital
Abstract
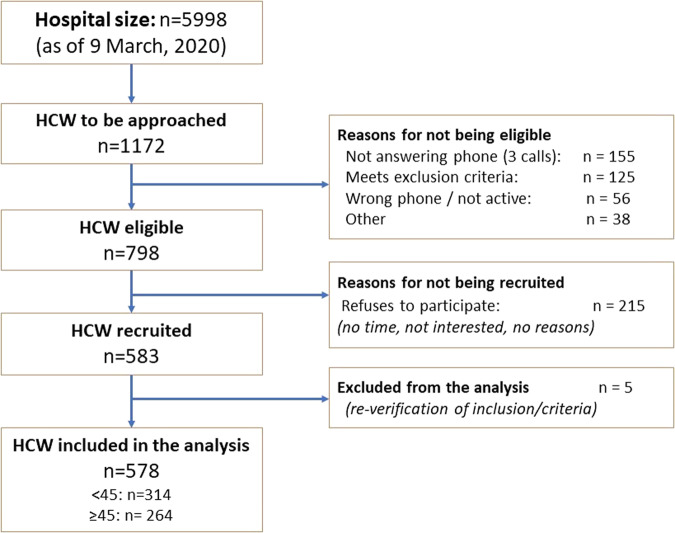
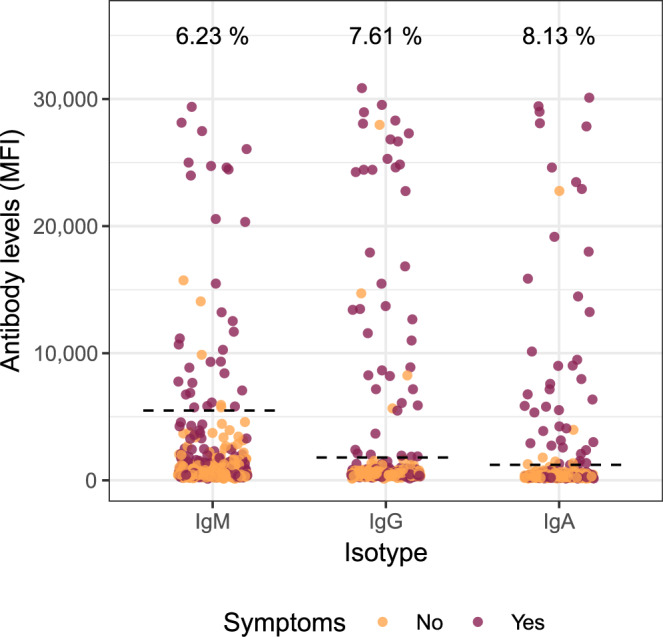
Health care workers (HCW) are a high-risk population to acquire SARS-CoV-2 infection from patients or other fellow HCW. This study aims at estimating the seroprevalence against SARS-CoV-2 in a random sample of HCW from a large hospital in Spain. Of the 578 participants recruited from 28 March to 9 April 2020, 54 (9.3%, 95% CI: 7.1-12.0) were seropositive for IgM and/or IgG and/or IgA against SARS-CoV-2. The cumulative prevalence of SARS-CoV-2 infection (presence of antibodies or past or current positive rRT-PCR) was 11.2% (65/578, 95% CI: 8.8-14.1). Among those with evidence of past or current infection, 40.0% (26/65) had not been previously diagnosed with COVID-19. Here we report a relatively low seroprevalence of antibodies among HCW at the peak of the COVID-19 epidemic in Spain. A large proportion of HCW with past or present infection had not been previously diagnosed with COVID-19, which calls for active periodic rRT-PCR testing in hospital settings.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19-. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re... (2020).
-
- Day, M. Covid-19: four fifths of cases are asymptomatic, China figures indicate. BMJ m1375. 10.1136/bmj.m1375 (2020). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
