

Prevalence and triggers of self-reported nasal hyperreactivity in adults with asthma
- PMID: 32642023
- PMCID: PMC7334478
- DOI: 10.1016/j.waojou.2020.100132
Prevalence and triggers of self-reported nasal hyperreactivity in adults with asthma
Abstract
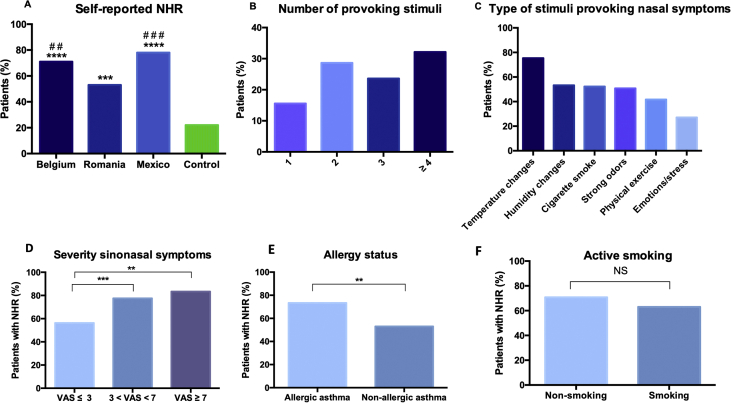
Background: Nasal hyperreactivity (NHR) is a common feature of various rhinitis subtypes and represents a novel phenotype of rhinitis. It is being reported in two-thirds of adult rhinitis patients irrespective of the atopic status. Data on the prevalence of NHR in patients with asthma are lacking, as well as the nature of evoking triggers.
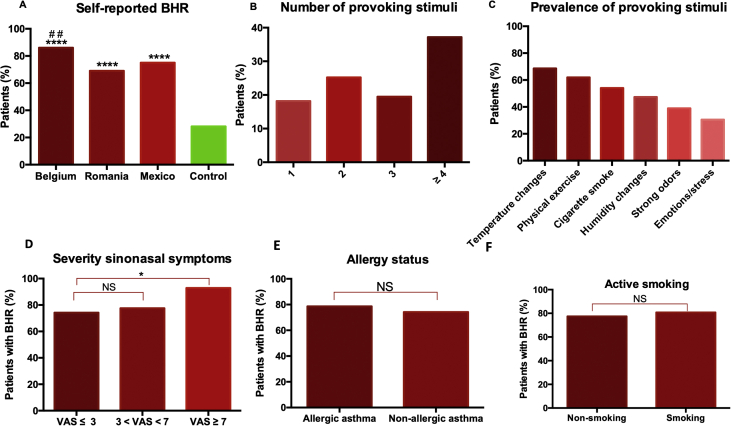
Methods: Postal questionnaires were distributed to an unselected group of asthmatic patients in Leuven (Belgium, n = 190) and completed by 114 patients. In Mexico City (Mexico) and Brasov (Romania), respectively, 97 out of 110 and 80 out of 100 asthmatic patients attending the outpatient clinic completed the questionnaire. Non-asthmatic volunteers were recruited amongst university and hospital co-workers in Leuven (n = 53). The presence of self-reported NHR, the type of triggers evoking nasal and bronchial symptoms, medication use, self-reported allergy, and environmental factors were evaluated.
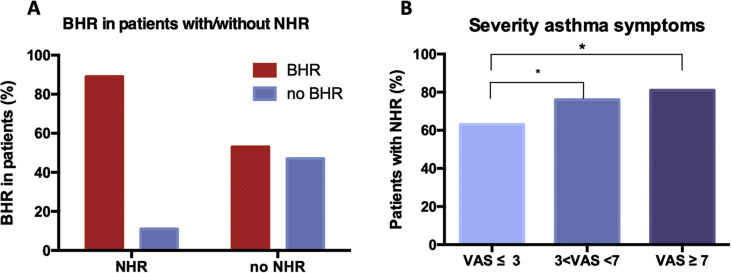
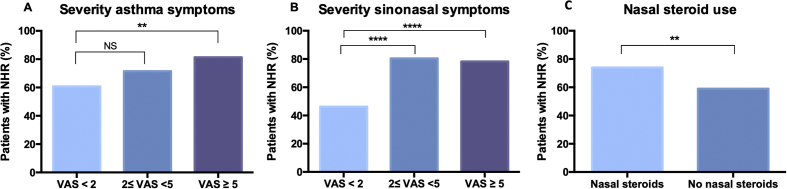
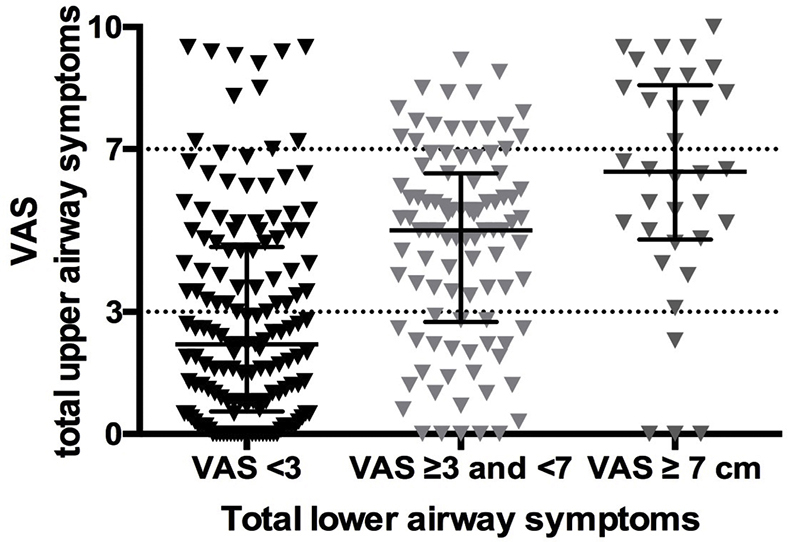
Results: Overall, 69% of asthma patients reported NHR, with 32% having more than 4 triggers evoking NHR. These triggers included mainly exposure to temperature and humidity changes, cigarette smoke, and strong odours. A higher prevalence of NHR was detected in allergic compared to non-allergic asthma patients (73% vs. 53% p < 0.01). The prevalence of NHR correlated with asthma severity, ranging from 63% (VAS ≤3) to 81% (VAS ≥7). BHR was found more frequently in patients with NHR compared to without NHR (89% vs. 53%, p < 0.0001).
Conclusion: NHR represents a clinical phenotype of upper airway disease affecting over two-thirds of asthma patients and correlates with asthma severity. Targeting NHR in patients with asthma is often overlooked and should be reinforced in the future to achieve better symptom control.
Keywords: AR, allergic rhinitis; Asthma; Atopy; BHR, bronchial hyperreactivity; Bronchial hyperreactivity; FEV1, forced expiratory volume in one second; NHR, nasal hyperreactivity; Nasal hyperreactivity; Symptom severity; VAS, visual analogue scale.
© 2020 The Authors.
Conflict of interest statement
All authors state they have no conflict of interest in relation to this study and the results described in the manuscript.
Figures
Similar articles
-
Nasal hyperreactivity in rhinitis: A diagnostic and therapeutic challenge.Allergy. 2018 Sep;73(9):1784-1791. doi: 10.1111/all.13453. Epub 2018 Apr 22. Allergy. 2018. PMID: 29624710 Review.
-
[Allergic rhinitis and bronchial hyperreactivity].Allergol Immunopathol (Madr). 2004 Nov-Dec;32(6):340-3. doi: 10.1016/s0301-0546(04)79266-6. Allergol Immunopathol (Madr). 2004. PMID: 15617661 Review. Spanish.
-
Allergic rhinitis phenotypes based on bronchial hyperreactivity to methacholine.Am J Rhinol Allergy. 2014 Nov-Dec;28(6):214-8. doi: 10.2500/ajra.2014.28.4124. Am J Rhinol Allergy. 2014. PMID: 25514477
-
A study of Spirometric parameters in non asthmatic allergic rhinitis.Heliyon. 2021 Oct 29;7(11):e08270. doi: 10.1016/j.heliyon.2021.e08270. eCollection 2021 Nov. Heliyon. 2021. PMID: 34820531 Free PMC article.
-
Nasal hyperreactivity in allergic rhinitis and chronic rhinosinusitis with polyps: a role for neuronal pathways.Rhinology. 2024 Jun 1;62(3):299-309. doi: 10.4193/Rhin23.287. Rhinology. 2024. PMID: 38372647
Cited by
-
Rare presence and function of neuroendocrine cells in the nasal mucosa.Front Immunol. 2024 Aug 7;15:1394539. doi: 10.3389/fimmu.2024.1394539. eCollection 2024. Front Immunol. 2024. PMID: 39176088 Free PMC article.
-
Multiple reasons underlaying uncontrolled disease in the majority of chronic rhinosinusitis patients.Front Allergy. 2022 Dec 13;3:1048385. doi: 10.3389/falgy.2022.1048385. eCollection 2022. Front Allergy. 2022. PMID: 36583193 Free PMC article.
-
A TRiP Through the Roles of Transient Receptor Potential Cation Channels in Type 2 Upper Airway Inflammation.Curr Allergy Asthma Rep. 2021 Mar 18;21(3):20. doi: 10.1007/s11882-020-00981-x. Curr Allergy Asthma Rep. 2021. PMID: 33738577 Free PMC article. Review.
-
The Use of Azelastine Hydrochloride/Fluticasone Propionate in the Management of Allergic Rhinitis in Asia: A Review.J Asthma Allergy. 2024 Jul 12;17:667-679. doi: 10.2147/JAA.S451733. eCollection 2024. J Asthma Allergy. 2024. PMID: 39045291 Free PMC article. Review.
References
-
- Cockcroft D.W., Davis B.E. Mechanisms of airway hyperresponsiveness. J Allergy Clin Immunol. 2006;118(3):551–559. - PubMed
-
- Capro R.O., Casaburi R., Coates A., Enright P., Hankinson J. American thoracic society guidelines for methacholine and exercise challenge. Crit Care Med. 1999;10 - PubMed
-
- Coates A.L., Wanger J., Cockcroft D.W. ERS technical standard on bronchial challenge testing: general considerations and performance of methacholine challenge tests. Eur Respir J. 2017;49(5):1–17. - PubMed
-
- Van Gerven L., Steelant B., Hellings P.W. Nasal hyperreactivity in rhinitis: a diagnostic and therapeutic challenge. Allergy. 2018;2 - PubMed
-
- Segboer C.L., Holland C.T., Reinartz S.M. Nasal hyper-reactivity is a common feature in both allergic and nonallergic rhinitis. Allergy. 2013;68(11):1427–1434. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
