

The arterial-ligation-alone method for identifying the intersegmental plane during thoracoscopic anatomic segmentectomy
- PMID: 32642139
- PMCID: PMC7330350
- DOI: 10.21037/jtd.2020.03.83
The arterial-ligation-alone method for identifying the intersegmental plane during thoracoscopic anatomic segmentectomy
Abstract
Background: Currently, methods for identifying the intersegmental plane during anatomical segmentectomy can be classified into 2 categories: the bronchial method and the vascular method. One of the vascular methods, the arterial-ligation-alone method, has not yet been validated or objectively evaluated in a large case series. We thus aimed to confirm that the arterial-ligation-alone method could effectively and accurately identify the intersegmental plane.
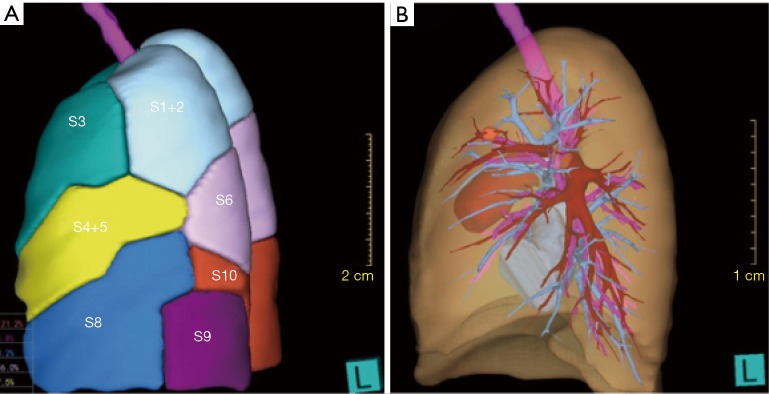
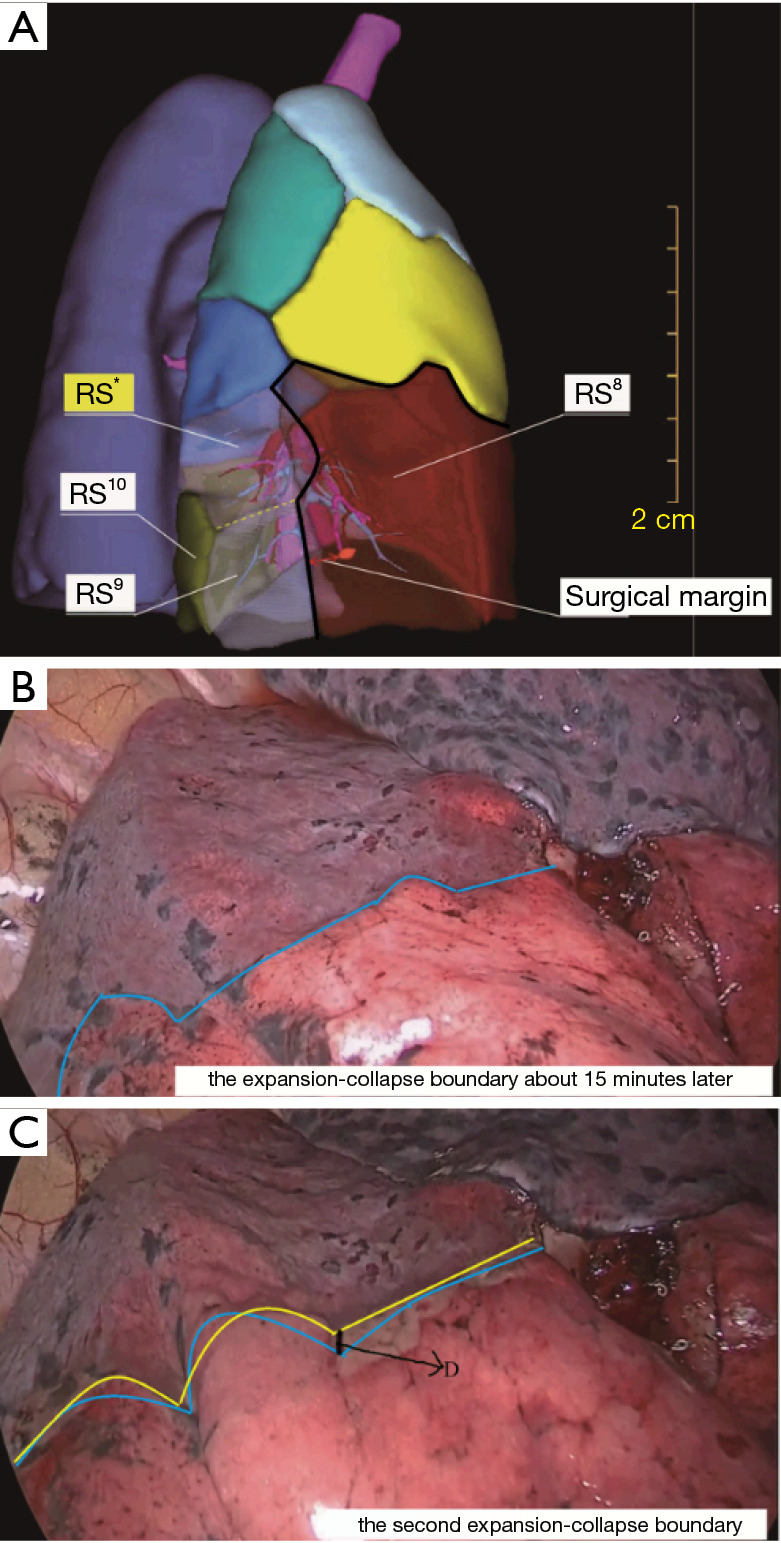
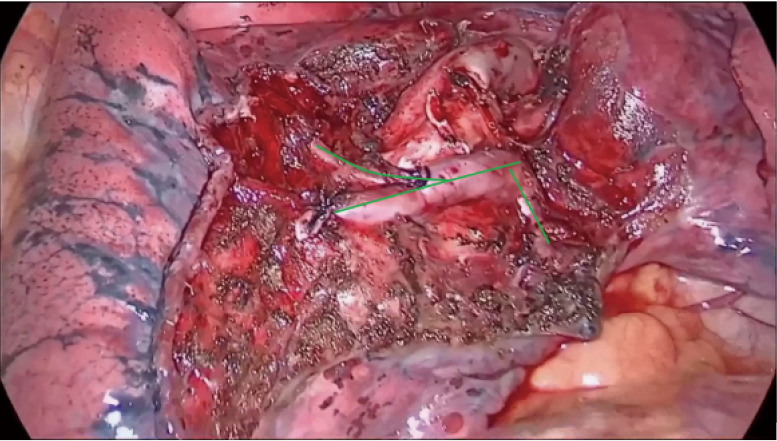
Methods: We retrospectively reviewed the records of 104 patients who were scheduled for thoracoscopic anatomic segmentectomy. Preoperative three-dimensional (3D) reconstruction was performed on all the affected lungs to distinguish the targeted segmental arteries, veins and bronchi. The procedure was as follows: first, based on the 3D reconstruction of the lung, the targeted segmental arteries were distinguished and ligated. Second, bilateral pulmonary ventilation was performed with pure oxygen. When the affected lung had completely inflated, contralateral pulmonary ventilation was performed. After waiting for some time, the first intersegmental plane could be obtained, and the time was recorded as T1, with an electric coagulation hook being used for marking. Thirdly, when the targeted segmental veins and bronchi had been ligated, the second intersegmental plane could be obtained by the inflation-deflation method as before, with the waiting time being recorded as T2. The differences between the 2 intersegmental planes were evaluated by 2 experienced chief thoracic surgeons.
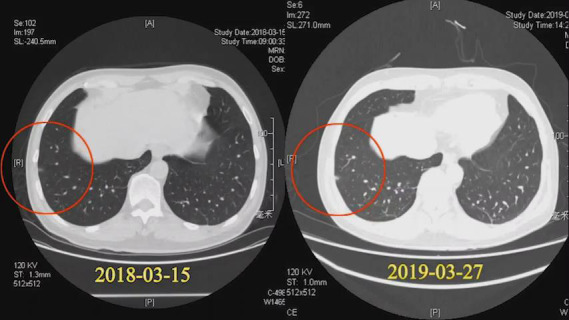
Result: In a total of 99 (95.2%) patients, the intersegmental planes were successfully and accurately identified by the arterial-ligation-alone method. Ultimately, 85 (81.7%) patients underwent thoracoscopic anatomic segmentectomy. The results for evaluating the differences between the 2 planes were as follows: completely consistent (94 cases, 94.9%), basically consistent (5 cases, 5.1%), and discrepant (0 cases, 0%). The mean T1 was 13.6±2.7 minutes (range, 8-25 minutes), and the mean T2 was 13.0±2.6 minutes (range, 8-23 minutes), with P=0.100 (95% CI). For 99 patients, the mean nodule size was 1.1±0.34 cm. In the 85 patients who underwent segmentectomy, the mean margin width was 2.84±0.51 cm, the mean operative duration was 165.6±18.3 minutes, the mean operative hemorrhage was 52.1±20.2 mL, and the mean duration of chest tube drainage was 3.9±1.3 days. Postoperative complications related to operative procedures occurred in 2 cases.
Conclusions: The arterial-ligation-only method can effectively, accurately and inexpensively identify the intersegmental plane, and is especially suitable for the patients whose veins or bronchi are difficult to anatomize. Whether the target bronchus is ligated has no effect on the intersegmental plane.
Keywords: Lung cancer; ground glass nodule; inflation-deflation method; three-dimensional reconstruction (3D reconstruction).
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd.2020.03.83). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources