

Subxiphoid completion thymectomy for refractory non-thymomatous myasthenia gravis
- PMID: 32642144
- PMCID: PMC7330301
- DOI: 10.21037/jtd.2020.03.81
Subxiphoid completion thymectomy for refractory non-thymomatous myasthenia gravis
Abstract
Background: Completion thymectomy may be performed in patients with non-thymomatous refractory myasthenia gravis (MG) to allow a complete and definitive clearance from residual thymic tissue located in the mediastinum or in lower neck. Hereby we present our short- and long-term results of completion thymectomy using subxiphoid video-assisted thoracoscopy.
Methods: Between July 2010 and December 2017, 15 consecutive patients with refractory non-thymomatous myasthenia, 8 women and 7 men with a median age of 44 [interquartile range (IQR) 38.5-53.5] years, underwent video-thoracoscopic completion thymectomy through a subxiphoid approach.
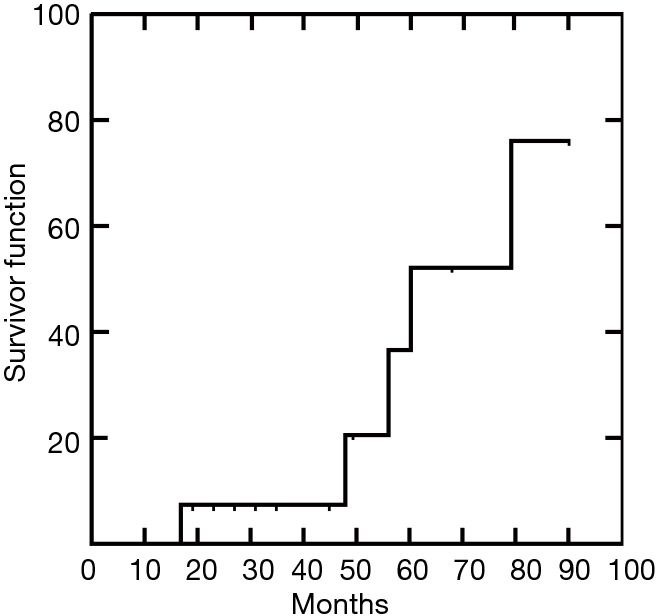
Results: Positron emission tomography (PET) showed mildly avid areas [standardized uptake value (SUV) more than or equal to 1.8] in 11 instances. Median operative time was 106 (IQR, 77-141) minutes. No operative deaths nor major morbidity occurred. Mean 1-day postoperative Visual Analogue Scale value was 2.53±0.63. Median hospital stay was 2 (IQR, 1-3.5) days. A significant decrease of the anti-acetylcholine receptor antibodies was observed after 1 month [median percentage changes -67% (IQR, -39% to -83%)]. Median follow-up was 45 (IQR, 21-58) months. At the most recent follow-up complete stable remission was achieved in 5 patients. Another 9 patients had significant improvement in bulbar and limb function, requiring lower doses of corticosteroids and anticholinesterase drugs. Only one patient remained clinically stable albeit drug doses were reduced. One-month postoperative drop of anti-acetylcholine receptor antibodies was significantly correlated with complete stable remission (P=0.002).
Conclusions: This initial experience confirms that removal of ectopic and residual thymus through a subxiphoid approach can reduce anti-acetylcholine receptor antibody titer correlating to good outcome of refractory MG.
Keywords: Myasthenia gravis (MG); acetylcholine receptor antibodies; completion thymectomy; subxiphoid video-assisted thoracic surgery (subxiphoid VATS).
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd.2020.03.81). The authors have no conflicts of interest to declare.
Figures



References
LinkOut - more resources
Full Text Sources