

Oncologic outcomes of lobectomy vs. segmentectomy in non-small cell lung cancer with clinical T1N0M0 stage: a literature review and meta-analysis
- PMID: 32642239
- PMCID: PMC7330803
- DOI: 10.21037/jtd-19-3802
Oncologic outcomes of lobectomy vs. segmentectomy in non-small cell lung cancer with clinical T1N0M0 stage: a literature review and meta-analysis
Abstract
Background: Lobectomy has long been regarded as the standard treatment for operable non-small cell lung cancer (NSCLC). Recent studies suggested that segmentectomy could achieve a good prognosis for early-stage NSCLC and might be an alternative to lobectomy in this cohort. Until now, on the issue of comparison between lobectomy and segmentectomy, there remains no published randomized controlled trial (RCT), and all existing evidence is low. Recently, a categorization of lower-level evidence has been proposed, namely, the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system. The aim of this meta-analysis is to compare the oncologic outcome between lobectomy and segmentectomy in NSCLC with the clinical T1N0M0 stage according to the GRADE system.
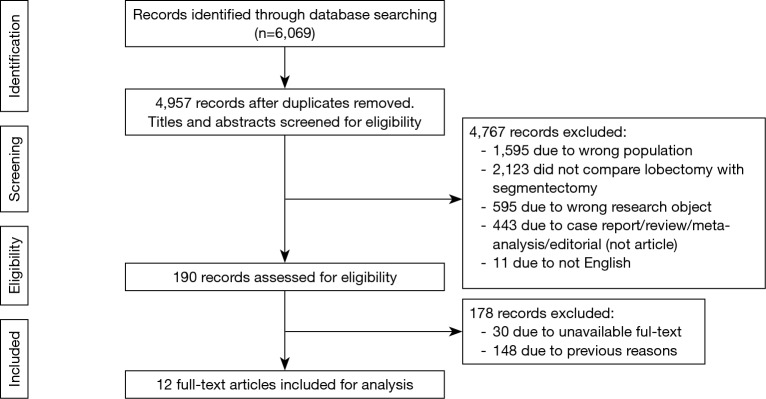
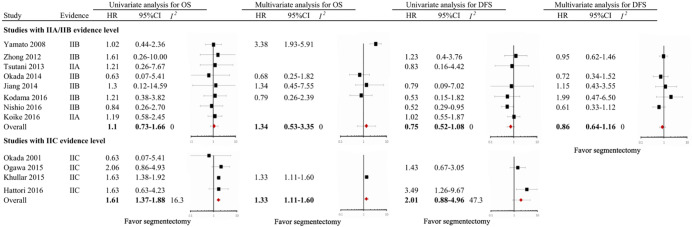
Methods: PubMed, the PMC database, EMBASE, Web of Science, and the Cochrane library were searched prior to May 2019 to identify studies that compared the prognosis between lobectomy and segmentectomy for clinical T1N0M0 NSCLC. The evidence level of the included studies was assessed according to the GRADE system, including level IIA, probably not confounded nonrandomized comparison; level IIB, possibly confounded nonrandomized comparison; and level IIC, probably confounded nonrandomized comparison. The predefined outcomes included overall survival (OS) and disease-free survival (DFS). Univariable and multivariable hazard ratios (HRs) with 95% confidence intervals (95% CI) were pooled using a random-effects model.
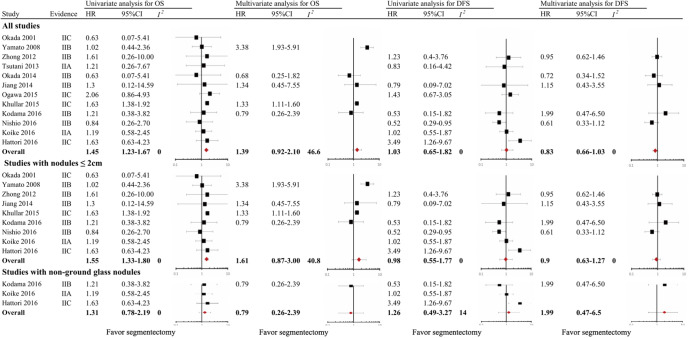
Results: Twelve nonrandomized studies involving 8,072 participants were included. Of these studies, two were classified as IIA level (16.7%), six as IIB level (50.0%), and four as IIC level (33.3%). When crude HRs were included, compared with lobectomy, segmentectomy was associated with shorter OS but comparable DFS in the entire cohort (OS, pooled HR =1.45, 95% CI, 1.23 to 1.67; DFS, pooled HR =1.03, 95% CI, 0.65 to 1.82) and in patients with nodules ≤2 cm (OS, pooled HR =1.55, 95% CI, 1.33 to 1.80; DFS, pooled HR =0.98, 95% CI, 0.55 to 1.77). When adjusted HRs were included, the impact of segmentectomy on OS and DFS was comparable to that of lobectomy in the entire cohort (OS, pooled HR =1.39, 95% CI, 0.92 to 2.10; DFS, pooled HR =0.83, 95% CI, 0.66 to 1.03) and in patients with nodules ≤2 cm (OS, pooled HR =1.61, 95% CI, 0.87 to 3.00; DFS, pooled HR =0.90, 95% CI, 0.63 to 1.27).
Conclusions: Based on our results, although shorter OS is observed in patients received segmentectomy, it is necessary to wait for more results from RCT to draw a valid conclusion.
Keywords: IA stage; Non-small cell lung cancer (NSCLC); clinical stage; lobectomy; meta-analysis; segmentectomy.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-19-3802). The authors have no conflicts of interest to declare.
Figures
References
-
- Liang W, He J, Shen Y, et al. Impact of Examined Lymph Node Count on Precise Staging and Long-Term Survival of Resected Non-Small-Cell Lung Cancer: A Population Study of the US SEER Database and a Chinese Multi-Institutional Registry. J Clin Oncol 2017;35:1162-70. 10.1200/JCO.2016.67.5140 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources