

MINOCA: The caveat of absence of coronary obstruction in myocardial infarction
- PMID: 32642553
- PMCID: PMC7334364
- DOI: 10.1016/j.ijcha.2020.100572
MINOCA: The caveat of absence of coronary obstruction in myocardial infarction
Abstract
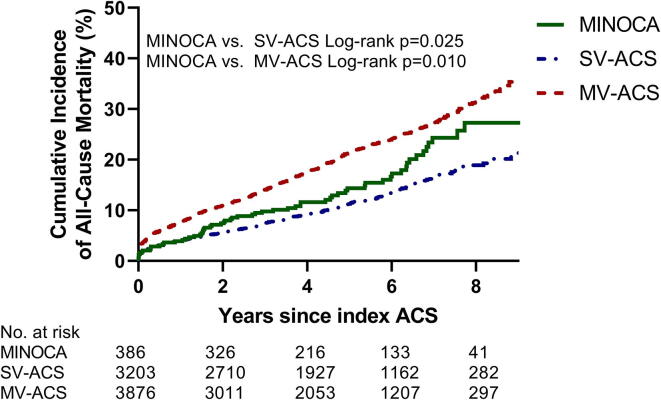
Aims: Whether patients with MINOCA (myocardial infarction with non-obstructive coronary arteries) have better outcomes than patients with obstructive coronary artery disease remains contradictory. The current study focussed on the clinical profile and prognosis of MINOCA patients.
Methods and results: We performed a retrospective analysis of patients with acute coronary syndrome (ACS) admitted to the Isala hospital in Zwolle, the Netherlands, between 2006 and 2014. A total of 7693 patients were categorized into three groups: MINOCA, single-vessel obstructive ACS (SV-ACS), and multi-vessel obstructive ACS (MV-ACS). MINOCA patients (5.2% of the total population) were more likely to be female (51.5% vs. 30.3% and 26.0% in SV-ACS and MV-ACS, respectively, p < 0.001 for both). The prevalence of risk factors in the MINOCA group was in between the SV-ACS and MV-ACS groups. Logistic regression revealed a lower odds of dying in SV-ACS (odds ratio (OR) = 0.70 (p = 0.04)) and a similar odds in MV-ACS (OR = 0.88, p = 0.45) compared to MINOCA.
Conclusions: Patients with MINOCA show an 'intermediate' risk profile with mortality rates in between those of both ACS groups. Hence, MINOCA should be recognised as a potential risk factor for mortality, requiring adequate treatment and follow-up.
Keywords: ACS/NSTE-ACS; Clinical research; MINOCA; STE-ACS.
© 2020 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relation which could have affected the work reported in this paper.
Figures
References
-
- Pasupathy S., Air T., Dreyer R.P., Tavella R., Beltrame J.F. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015;131:861–870. - PubMed
-
- Agewall S., Beltrame J.F., Reynolds H.R. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. 2017;38:143–153. - PubMed
-
- Tamis-Holland J.E., Jneid H., Reynolds H.R. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation. 2019;139:e891–e908. - PubMed
-
- Sharifi M., Frohlich T.G., Silverman I.M. Myocardial infarction with angiographically normal coronary arteries. Chest. 1995;107:36–40. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
