

Constitutional mismatch repair deficiency-associated brain tumors: report from the European C4CMMRD consortium
- PMID: 32642664
- PMCID: PMC7212899
- DOI: 10.1093/noajnl/vdz033
Constitutional mismatch repair deficiency-associated brain tumors: report from the European C4CMMRD consortium
Abstract
Background: Malignant brain tumors (BT) are among the cancers most frequently associated with constitutional mismatch repair deficiency (CMMRD), a rare childhood cancer predisposition syndrome resulting from biallelic germline mutations in mismatch repair genes. This study analyzed data from the European "Care for CMMRD" (C4CMMRD) database to describe their clinical characteristics, treatments, and outcome with the aim of improving its diagnosis/treatment.
Methods: Retrospective analysis of data on patients with CMMRD and malignant BT from the C4CMMRD database up to July 2017.
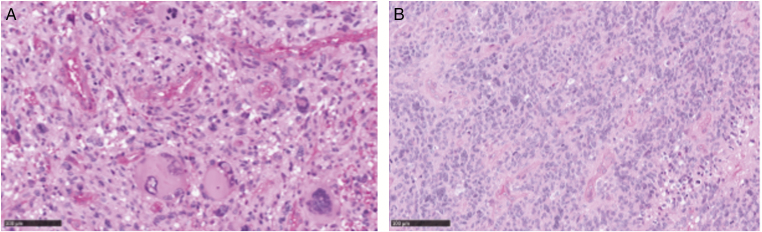
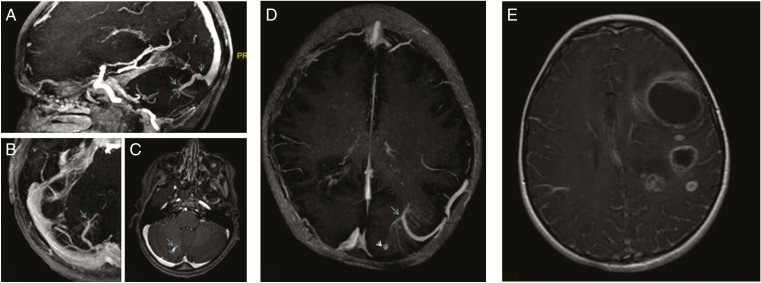
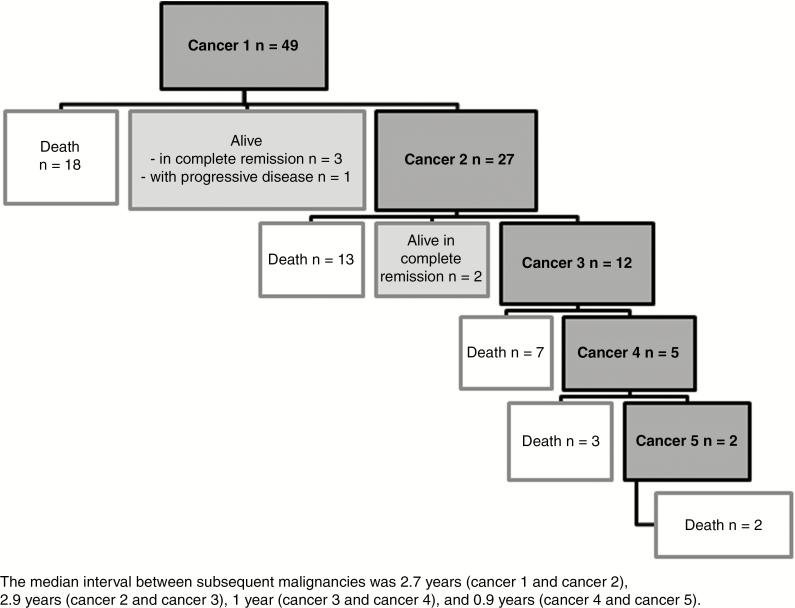
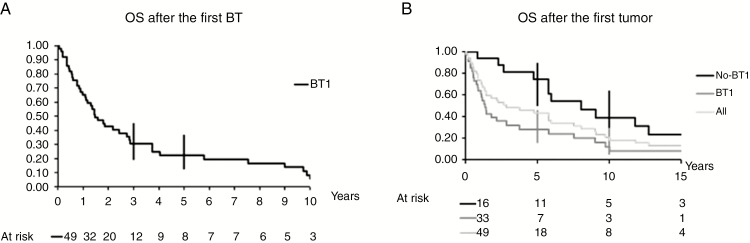
Results: Among the 87 registered patients, 49 developed 56 malignant BTs: 50 high-grade gliomas (HGG) (with giant multinucleated cells in 16/21 histologically reviewed tumors) and 6 embryonal tumors. The median age at first BT was 9.2 years [1.1-40.6], with nine patients older than 18. Twenty-seven patients developed multiple malignancies (including16 before the BT). Most patients received standard treatment, and eight patients immunotherapy for relapsed HGG. The 3- and 5-year overall survival (OS) rates were 30% (95% CI: 19-45) and 22% (95% CI: 12-37) after the first BT, with worse prognosis for HGG (3-year OS = 20.5%). Six patients were alive (median follow-up 2.5 years) and 43 dead (38 deaths, 88%, were BT-related). Other CMMRD-specific features were café-au-lait macules (40/41), multiple BTs (5/15), developmental brain anomalies (11/15), and consanguinity (20/38 families).
Conclusions: Several characteristics could help suspecting CMMRD in pediatric malignant BTs: giant cells on histology, previous malignancies, parental consanguinity, café-au-lait macules, multiple BTs, and developmental brain anomalies. The prognosis of CMMRD-associated BT treated with standard therapies is poor requiring new therapeutic up-front approaches.
Keywords: MMR biallelic germline mutation; brain tumor; café-au-lait spot; childhood cancer; constitutional mismatch repair deficiency; high-grade glioma; predisposition.
© The Author(s) 2019. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
References
-
- Kunkel TA, Erie DA. DNA mismatch repair. Annu Rev Biochem. 2005;74:681–710. - PubMed
-
- Wang Q, Lasset C, Desseigne F, et al. Neurofibromatosis and early onset of cancers in hMLH1-deficient children. Cancer Res. 1999;59(2): 294–297. - PubMed
-
- Ricciardone MD, Ozçelik T, Cevher B, et al. Human MLH1 deficiency predisposes to hematological malignancy and neurofibromatosis type 1. Cancer Res. 1999;59(2):290–293. - PubMed
-
- Wimmer K, Kratz CP, Vasen HFA, et al. Diagnostic criteria for constitutional mismatch repair deficiency syndrome: suggestions of the European consortium “care for CMMRD” (C4CMMRD). J Med Genet. 2014;51(6):355–365. - PubMed
LinkOut - more resources
Full Text Sources