

Bevacizumab-based treatment as salvage therapy in patients with recurrent symptomatic brain metastases
- PMID: 32642693
- PMCID: PMC7212911
- DOI: 10.1093/noajnl/vdaa038
Bevacizumab-based treatment as salvage therapy in patients with recurrent symptomatic brain metastases
Abstract
Background: Salvage treatment for recurrent brain metastases (BM) of solid cancers is challenging due to the high symptomatic burden and the limited local treatment options.
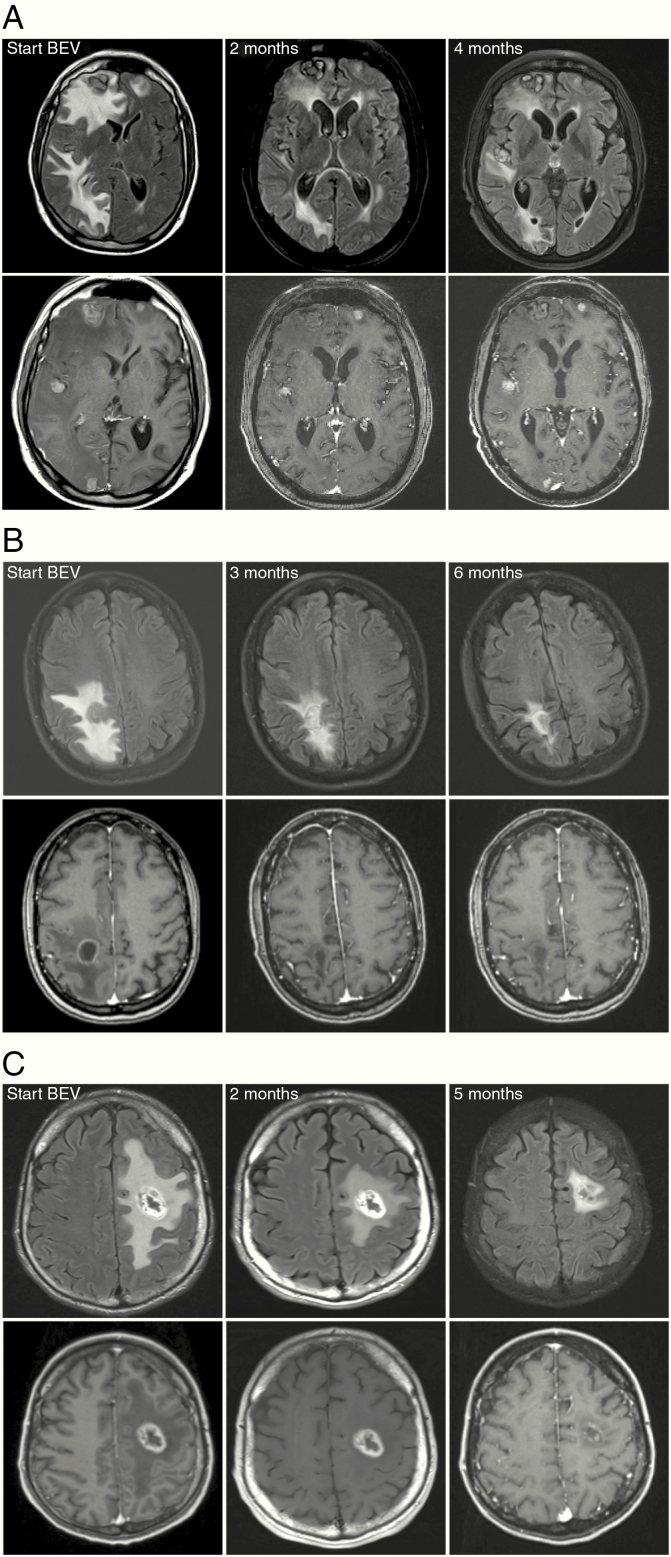
Methods: Patients with recurrent BM with no option for further local therapies were retrospectively identified from BM databases. Bevacizumab-based treatment was initiated as a salvage treatment. Radiological imaging before and after bevacizumab-based treatment was reevaluated for treatment response using the Response Assessment in Neuro-Oncology (RANO) BM criteria.
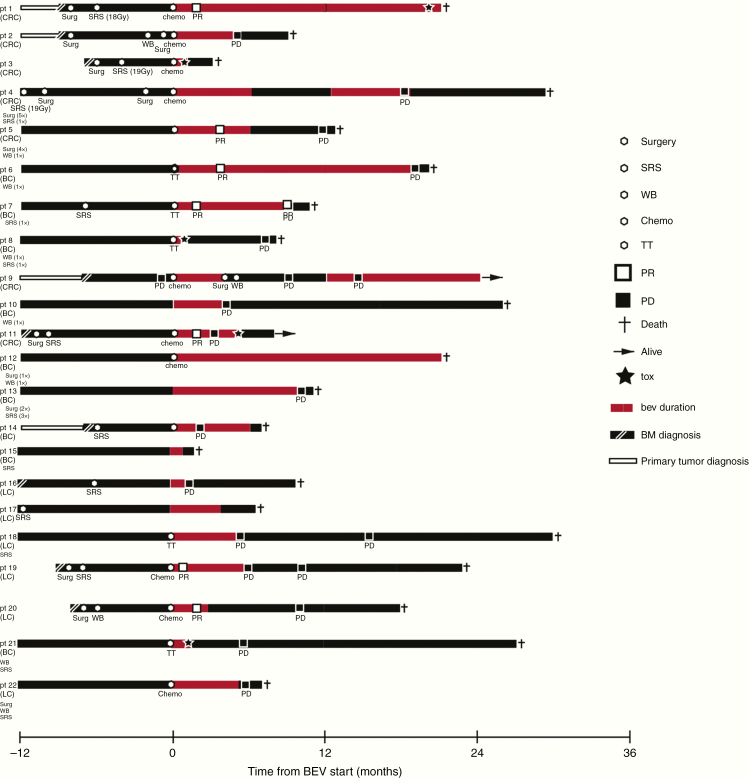
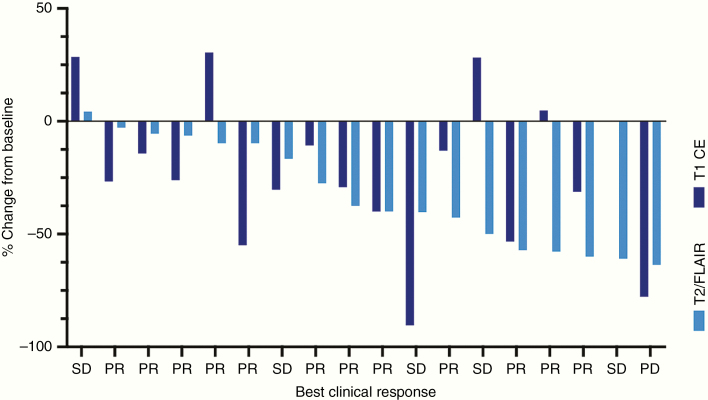
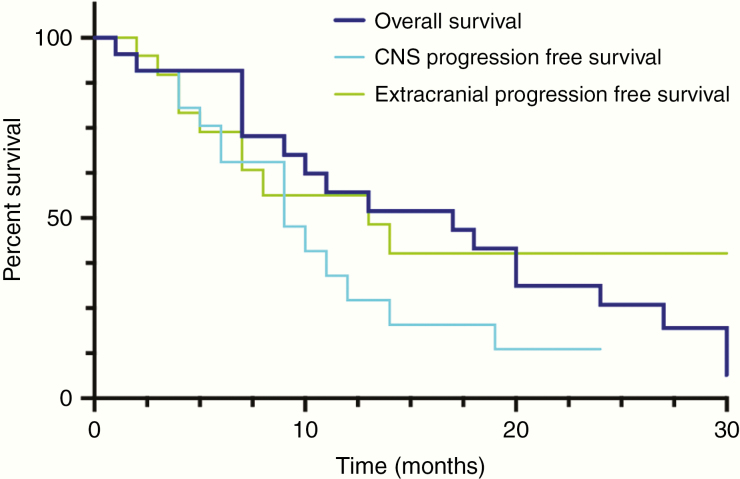
Results: Twenty-two patients (36.4% male) with recurrent BM from breast cancer (40.9%), colorectal cancer (31.8%), or lung cancer (27.3%) were identified. Previous BM-directed therapies were radiosurgery in 16/22 (72.7%) patients, whole-brain radiotherapy in 8/22 (36.4%), and neurosurgical resection in 11/22 (50.0%). Time since BM diagnosis to initiation of bevacizumab treatment was 16.5 months. Of 22 patients 14 (63.6%) received concurrent systemic therapies. Neurological symptom improvement could be achieved in 14/22 (63.6%) and stabilization in 6/22 (27.3%) patients, resulting in a clinical benefit in 20/22 (90.9%) patients. Steroids could be reduced or stopped in 15/22 (68.2%) patients. Rate of improvement on T1-weighted imaging was 15/19 (78.9%; median reduction: -26.0% ± 32.9) and 19/20 (95%; median reduction: -36.2% ± 22.2) on T2-weighted FLAIR imaging. According to RANO-BM best response was partial response in 7/19 (36.8%), stable disease in 9/19 (47.3%), and progressive disease in 3/19 (15.7%) patients. Median CNS-specific progression-free survival was 8 months and median overall survival after initiation of bevacizumab treatment was 17 months.
Conclusions: Bevacizumab-based treatment had clinically relevant intracranial activity in the vast majority of patients suffering from recurrent, symptomatic BM. The data supports a prospective clinical trial of bevacizumab as a salvage treatment in BM.
Keywords: bevacizumab; brain edema; brain metastases; recurrence; steroids.
© The Author(s) 2020. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
References
LinkOut - more resources
Full Text Sources