

Temporal patterns and short-term progression of paroxysmal atrial fibrillation: data from RACE V
- PMID: 32642768
- PMCID: PMC7400474
- DOI: 10.1093/europace/euaa123
Temporal patterns and short-term progression of paroxysmal atrial fibrillation: data from RACE V
Abstract
Aims: Atrial fibrillation (AF) often starts as a paroxysmal self-terminating arrhythmia. Limited information is available on AF patterns and episode duration of paroxysmal AF. In paroxysmal AF patients, we longitudinally studied the temporal AF patterns, the association with clinical characteristics, and prevalence of AF progression.
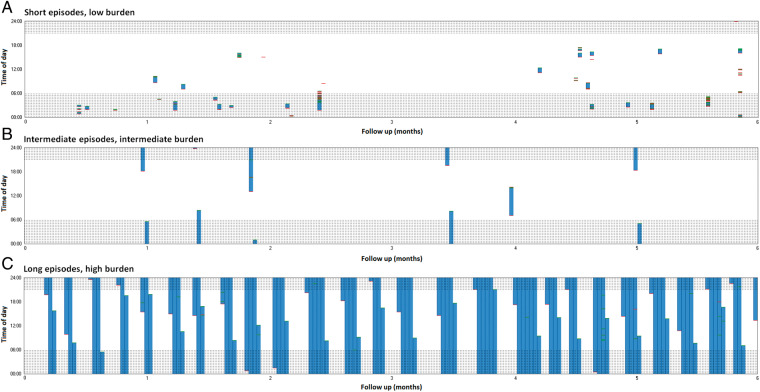
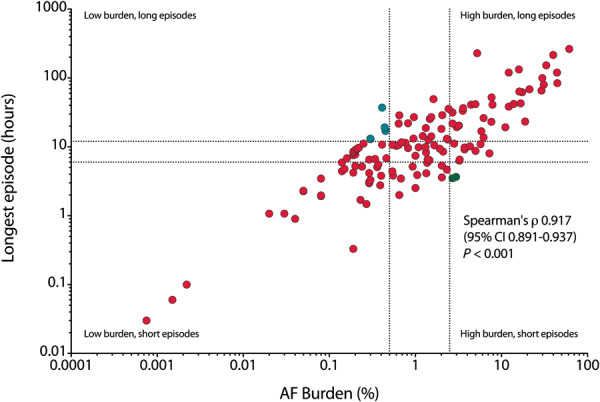
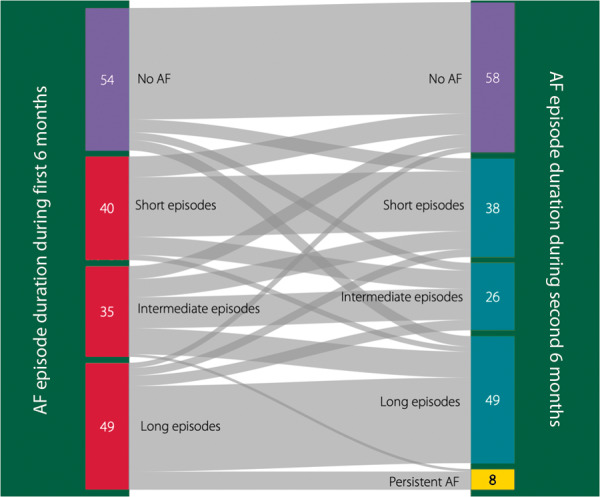
Methods and results: In this interim analysis of the Reappraisal of AF: Interaction Between HyperCoagulability, Electrical Remodelling, and Vascular Destabilisation in the Progression of AF (RACE V) registry, 202 patients with paroxysmal AF were followed with continuous rhythm monitoring (implantable loop recorder or pacemaker) for 6 months. Mean age was 64 ± 9 years, 42% were women. Atrial fibrillation history was 2.1 (0.5-4.4) years, CHA2DS2-VASc 1.9 ± 1.3, 101 (50%) had hypertension, 69 (34%) heart failure. One-third had no AF during follow-up. Patients with long episodes (>12 hours) were often men with more comorbidities (heart failure, coronary artery disease, higher left ventricular mass). Patients with higher AF burden (>2.5%) were older with more comorbidities (worse renal function, higher calcium score, thicker intima media thickness). In 179 (89%) patients, 1-year rhythm follow-up was available. On a quarterly basis, average daily AF burden increased from 3.2% to 3.8%, 5.2%, and 6.1%. Compared to the first 6 months, 111 (62%) patients remained stable during the second 6 months, 39 (22%) showed progression to longer AF episodes, 8 (3%) developed persistent AF, and 29 (16%) patients showed AF regression.
Conclusions: In paroxysmal AF, temporal patterns differ suggesting that paroxysmal AF is not one entity. Atrial fibrillation burden is low and determined by number of comorbidities. Atrial fibrillation progression occurred in a substantial number.
Trial registration number: Clinicaltrials.gov identifier NCT02726698.
Keywords: Atrial fibrillation; Atrial fibrillation burden; Atrial fibrillation progression; Paroxysmal atrial fibrillation; Rhythm monitoring.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- De Vos CB, Pisters R, Nieuwlaat R, Prins MH, Tieleman RG, Coelen RJ. et al. Progression from paroxysmal to persistent atrial fibrillation clinical correlates and prognosis. J Am Coll Cardiol 2010;55:725–31. - PubMed
-
- Nattel S, Guasch E, Savelieva I, Cosio FG, Valverde I, Halperin JL. et al. Early management of atrial fibrillation to prevent cardiovascular complications. Eur Heart J 2014;35:1448–56. - PubMed
-
- Steinberg BA, Hellkamp AS, Lokhnygina Y, Patel MR, Breithardt G, Hankey GJ, et al.; ROCKET-AF Steering Committee and Investigators. Higher risk of death and stroke in patients with persistent vs. paroxysmal atrial fibrillation: results from the ROCKET-AF Trial. Eur Heart J 2015;36:288–96. - PMC - PubMed
-
- Wong JA, Conen D, Van Gelder IC, McIntyre WF, Crijns HJ, Wang J. et al. Progression of device-detected subclinical atrial fibrillation and the risk of heart failure. J Am Coll Cardiol 2018;71:2603–11. - PubMed
-
- Vanassche T, Lauw MN, Eikelboom JW, Healey JS, Hart RG, Alings M, Avezum A. et al. Risk of ischaemic stroke according to pattern of atrial fibrillation: analysis of 6563 aspirin-treated patients in ACTIVE-A and AVERROES. Eur Heart J 2015;36:281–7a. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
