

Population Pharmacokinetics of Magnesium Sulfate in Preeclampsia and Associated Factors
- PMID: 32642964
- PMCID: PMC7419390
- DOI: 10.1007/s40268-020-00315-2
Population Pharmacokinetics of Magnesium Sulfate in Preeclampsia and Associated Factors
Abstract
Background and objective: The pharmacokinetic basis of magnesium sulphate (MgSO4) dosing regimens for preeclampsia (PE) prophylaxis and treatment is not clearly established. The aim of study is to develop a population pharmacokinetic (PK) model of MgSO4 in PE, and to determine key covariates having an effect in MgSO4 pharmacokinetics in preeclampsia (PE) and to determine key covariates having an effect in MgSO4 PK.
Methods: A prospective cohort study was conducted from June 2016 to February 2018 in patients with PE administered MgSO4 as a 4-g bolus followed by continuous infusion at a rate of 1 g/h. Serum magnesium concentrations were obtained before treatment administration and 2, 6, 12, and 18 h after the initial dose. The software Monolix was used to estimate population PK parameters of MgSO4 [clearance (CL), volume of distribution (V), half-life] and to develop a PK model with baseline patient demographic, clinical, and laboratory covariates.
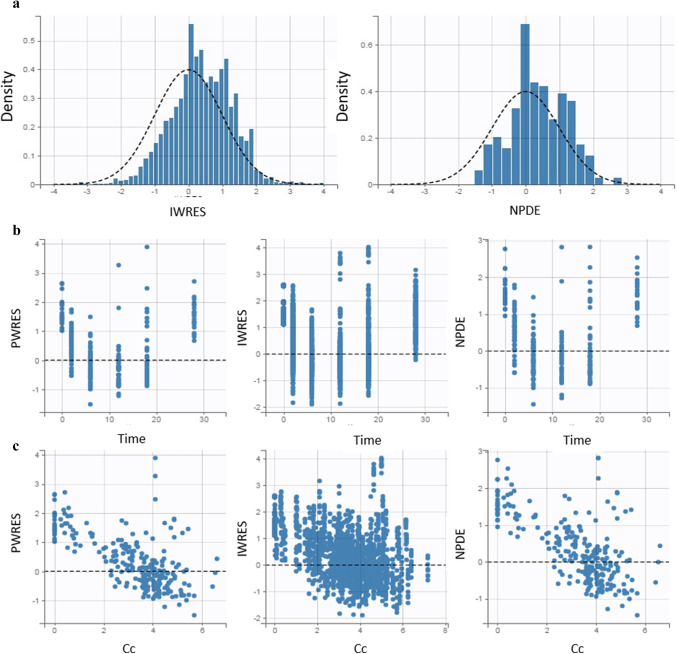
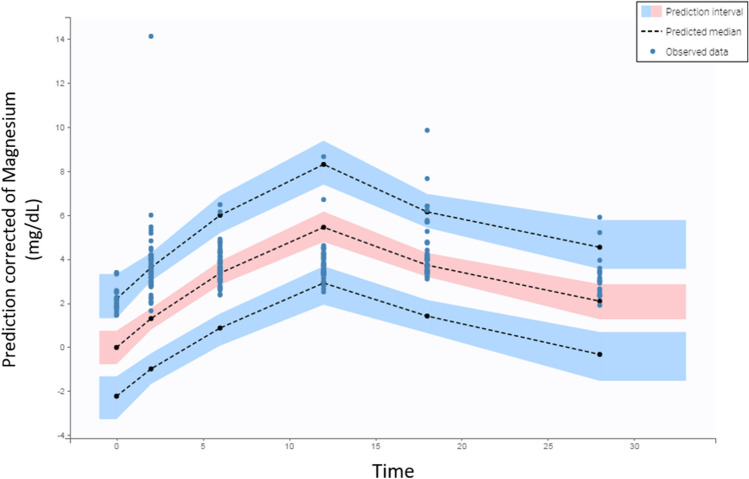
Results: The study population consisted of 109 patients. The PK profile of MgSO4 was adequately described by a one-compartment PK model. The model estimate of the population CL was 1.38 L/h; for V, it was 13.3 L; and the baseline magnesium concentration was 0.77 mmol/L (1.87 mg/dL). The baseline body weight and serum creatinine statistically influenced MgSO4 CL and V, respectively. The model was parameterized as CL and V.
Conclusion: The PK of MgSO4 in pregnant women with PE is significantly affected by creatinine and body weight. Pregnant women with PE and higher body weight have a higher V and, consequently, a lower elimination rate of MgSO4. Pregnant women with PE and a higher serum creatinine value show lower CL and, therefore, lower MgSO4 elimination rate.
Conflict of interest statement
The authors, Tatiana Xavier da Costa, Francine Johansson Azeredo, Marcela Abbott Galvão Ururahy, Miguel Adelino da Silva Filho, Rand Randall Martins, and Antonio Gouveia Oliveira, declare that there is no conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
