

Operative timing is associated with increased morbidity and mortality in patients undergoing emergency general surgery: a multisite study of emergency general services in a single academic network
- PMID: 32644317
- PMCID: PMC7458678
- DOI: 10.1503/cjs.012919
Operative timing is associated with increased morbidity and mortality in patients undergoing emergency general surgery: a multisite study of emergency general services in a single academic network
Abstract
Background: Despite the widespread implementation of the acute care surgery (ACS) model, limited access to operating room time represents a barrier to the optimal delivery of emergency general surgery (EGS) care. The objective of this study was to describe the effect of operative timing on outcomes in EGS in a network of teaching hospitals.
Methods: We conducted a retrospective review of EGS operations performed at 3 teaching hospitals in a single academic network. Time of operation was categorized as daytime (8 am to 5 pm), after hours (5 pm to 11 pm) or overnight (11 pm to 8 am). Time to operation was calculated as the interval from admission to operative start time and categorized as less than 24 hours, 24-72 hours and greater than 72 hours.
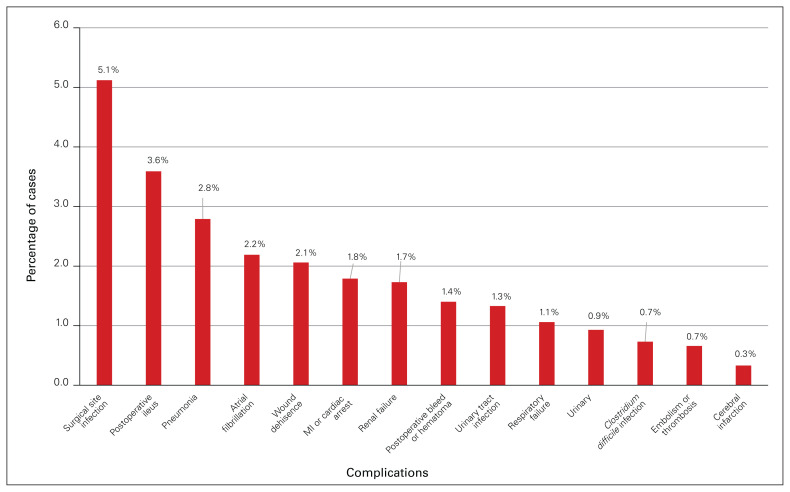
Results: After we excluded nonindex cases, trauma cases and cases occurring more than 5 days after admission, 1505 EGS cases were included. We found that 39.0% of operations were performed in the daytime, 46.3% after hours and 14.8% overnight. In terms of time to operation, 52.3% of operations were performed within 24 hours of admission, 33.4% in 24-72 hours and 14.3% in more than 72 hours. The overall complication rate was 20.6% (310 patients) and the overall mortality rate was 3.8% (57 patients). After multivariable analysis, time to operation more than 72 hours after admission was independently associated with increased odds of morbidity (odds ratio [OR] 1.64, 95% confidence interval [CI] 1.09-2.47), while overnight operating was associated with increased odds of death (OR 3.15, 95% CI 1.29-7.70).
Conclusion: Increasing time from admission to operation and overnight operating were associated with greater morbidity and mortality, respectively, for EGS patients. Strategies to provide timely access to the operating room should be considered to optimize care in an ACS model.
Contexte: Même si le modèle de chirurgie en soins actifs (CSA) est largement répandu, l’accès limité aux blocs opératoires représente un obstacle à la chirurgie générale chez les patients des services d’urgence (CGSU). L’objectif de cette étude était de décrire l’effet du moment de l’intervention sur l’issue des CGSU dans un réseau d’hôpitaux universitaires.
Méthodes: Nous avons procédé à une revue des CGSU effectuées dans 3 hôpitaux d’enseignement d’un réseau universitaire. Le moment opératoire était catégorisé selon que les interventions étaient effectuées le jour (8 h 00 à 17 h 00), le soir (17 h 00 à 23 h 00) ou la nuit (23 h 00 à 8 h 00). Le délai opératoire représentait l’intervalle entre l’admission et le début de l’intervention et était réparti selon les catégories suivantes : moins de 24 heures, de 24 à 72 heures et plus de 72 heures.
Résultats: Après exclusion des cas non index, des cas de traumatologie et des cas survenus plus de 5 jours après l’admission, 1505 CGSU ont été incluses. Nous avons constaté que 39,0 % des interventions avaient été effectuées le jour, 46,3 % le soir et 14,8 % la nuit. Pour ce qui est du délai opératoire, 52,3 % des interventions ont été effectuées dans les 24 heures suivant l’admission, 33,4 % dans les 24 à 72 heures et 14,3 % plus de 72 heures après l’admission. Le taux global de complications a été de 20,6 % (310 patients) et le taux de mortalité global a été de 3,8 % (57 patients). Après analyse multivariée, le délai opératoire de plus de 72 heures suivant l’admission a été associé de manière indépendante à un risque accru de morbidité (rapport ces cotes [RC] 1,64, intervalle de confiance [IC]) de 95 % 1,09 à 2,47), tandis que les interventions effectuées la nuit ont été associées à un risque de décès plus élevé (RC 3,15, IC de 95 % 1,29 à 7,70).
Conclusion: L’augmentation du délai entre l’admission et l’intervention et les interventions de nuit ont été associées à une morbidité et une mortalité plus élevées, respectivement, chez les patients soumis à des CGSU. Des stratégies visant à offrir un accès rapide aux blocs opératoires sont à envisager pour optimiser le modèle de CSA.
© 2020 Joule Inc. or its licensors.
Conflict of interest statement
T. Rice has received speaker fees from Cook Medical. No other competing interests were declared.
Figures


References
-
- Schaetzel S, Dirks R, Davis J. Comparison of outcomes of patients with acute appendicitis between an acute care surgery model and traditional call coverage model in the same community. Am J Surg. 2016;212:1083–9. - PubMed
-
- Britt RC, Bouchard C, Weireter LJ, et al. Impact of acute care surgery on biliary disease. J Am Coll Surg. 2010;210:595–9. 599–601. - PubMed
-
- Cubas RF, Gómez NR, Rodriguez S, et al. Outcomes in the management of appendicitis and cholecystitis in the setting of a new acute care surgery service model: impact on timing and cost. J Am Coll Surg. 2012;215:715–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical