

Clinical Effectiveness of Lumacaftor/Ivacaftor in Patients with Cystic Fibrosis Homozygous for F508del-CFTR. A Clinical Trial
- PMID: 32644818
- PMCID: PMC7780982
- DOI: 10.1513/AnnalsATS.202002-144OC
Clinical Effectiveness of Lumacaftor/Ivacaftor in Patients with Cystic Fibrosis Homozygous for F508del-CFTR. A Clinical Trial
Abstract
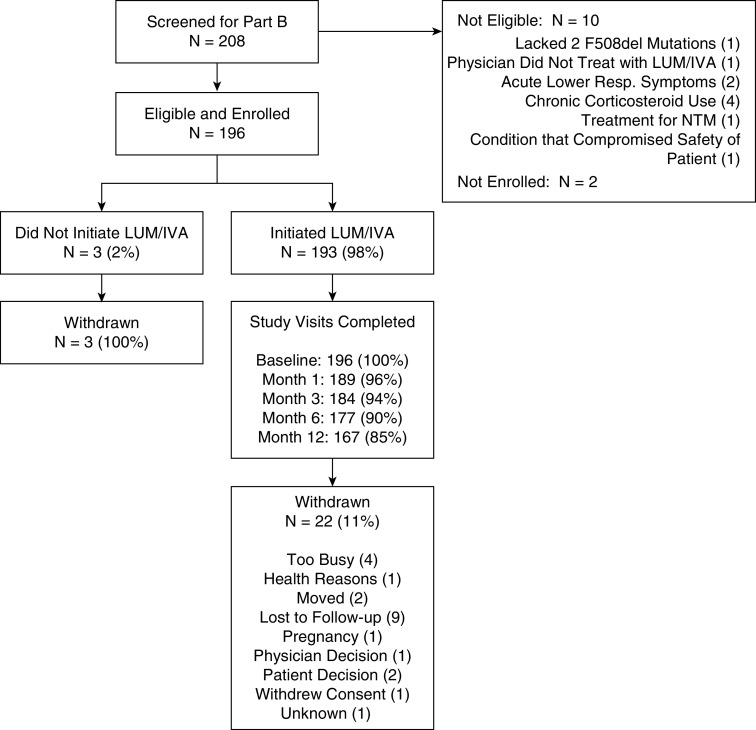
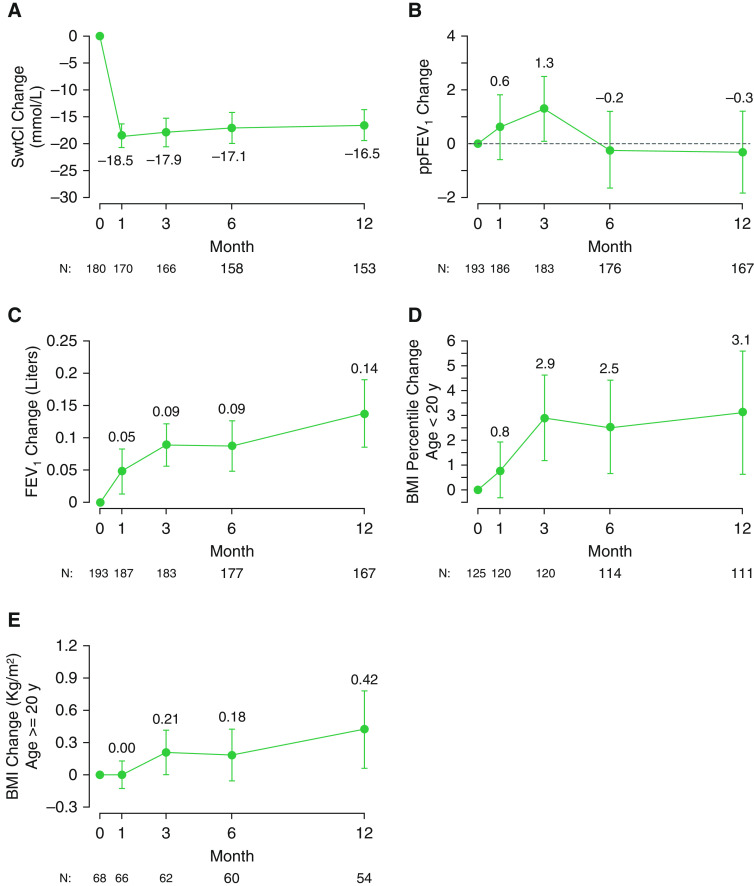
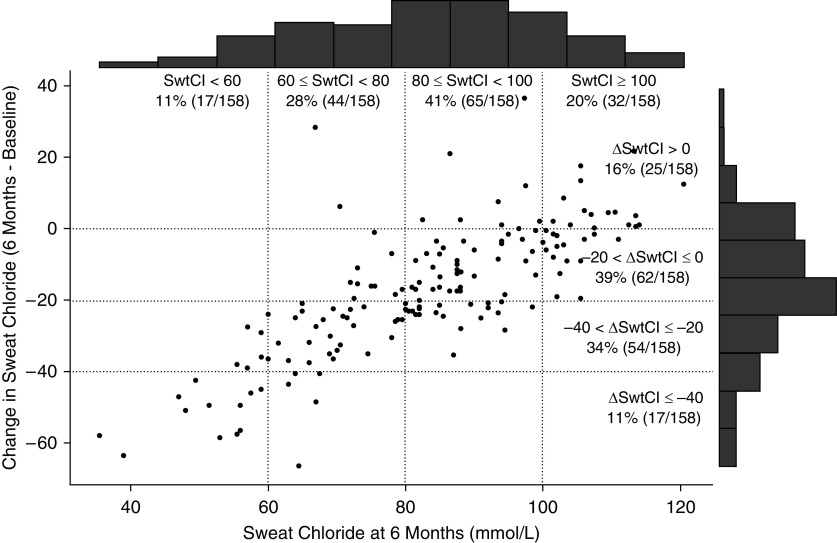
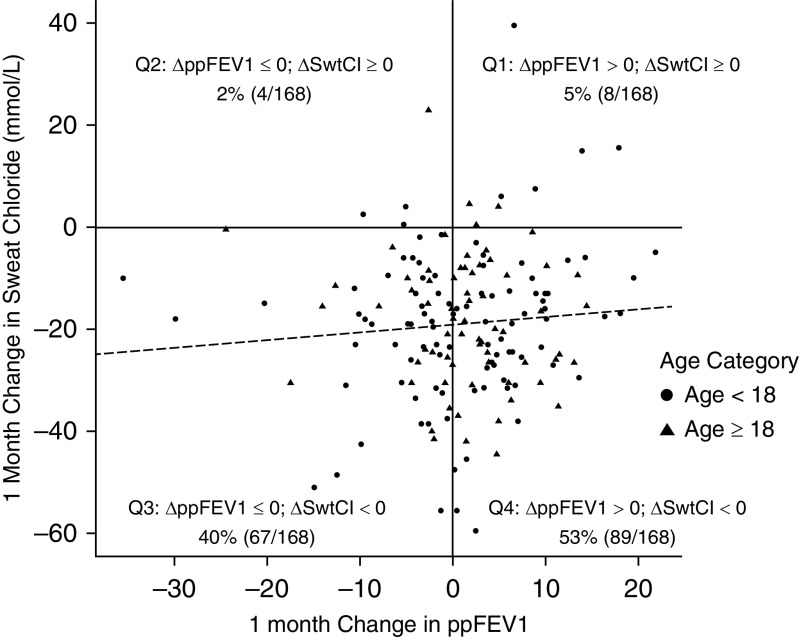
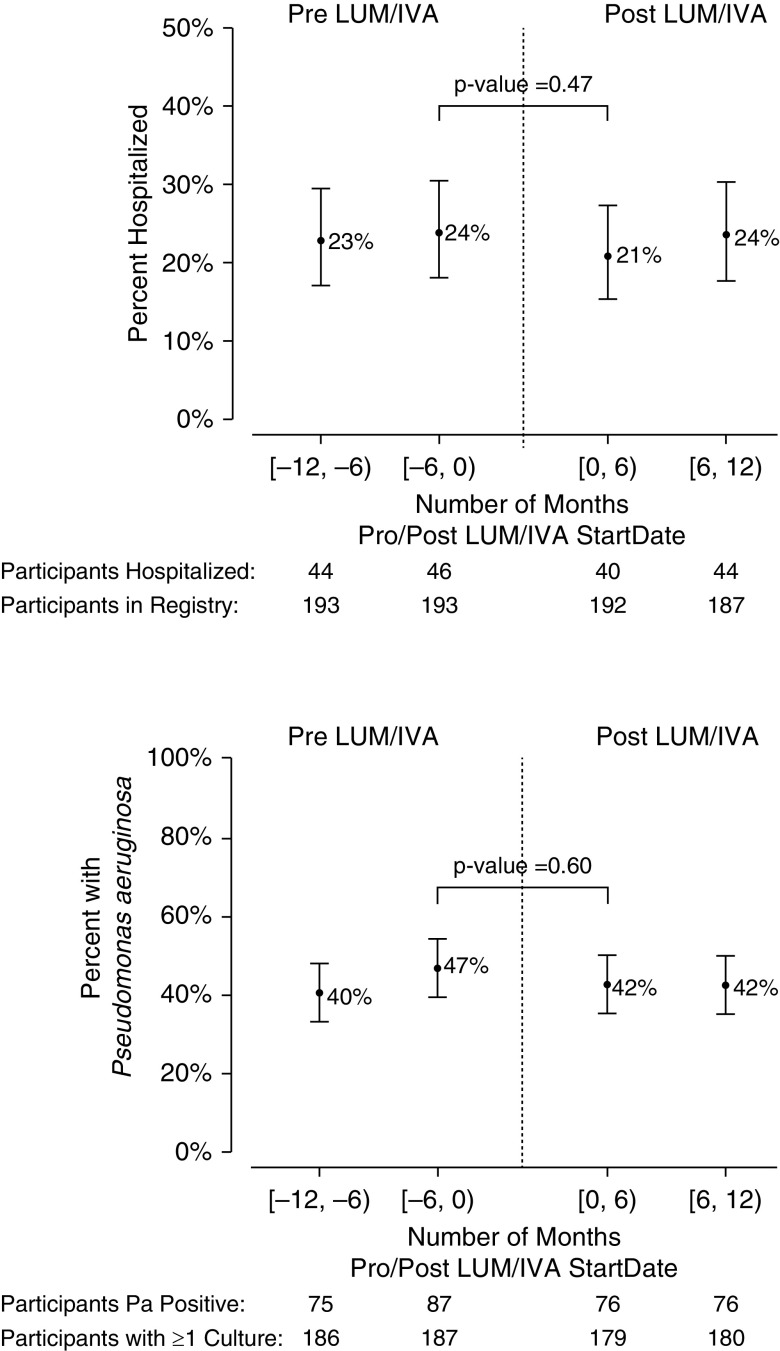
Rationale: The combination of lumacaftor (LUM) and ivacaftor (IVA) is an approved CFTR (cystic fibrosis [CF] transmembrane conductance regulator) modulator treatment for homozygous F508del patients with CF.Objectives: To evaluate the effectiveness of LUM/IVA in children (6 yr or more) and adults (more than 18 yr) in a postapproval setting.Methods: This longitudinal cohort study, performed at 38 centers in the U.S. CF Therapeutics Development Network, enrolled homozygous F508del patients with CF ages 6 years old and older with no prior exposure to LUM/IVA. Study assessments were performed at baseline and at 1, 3, 6, and 12 months after LUM/IVA initiation.Results: A total of 193 patients initiated LUM/IVA, and 85% completed the study through 1 year. Baseline mean percent-predicted forced expiratory volume in 1 second (ppFEV1) was 85 (standard deviation, 22.4) in this cohort. No statistically significant change in ppFEV1 was observed from baseline to any of the follow-up time points, with a mean absolute change at 12 months of -0.3 (95% confidence interval [CI], -1.8 to 1.2). Body mass index improved from baseline to 12 months (mean change, 0.8 kg/m2; P < 0.001). Sweat chloride decreased from baseline to 1 month (mean change, -18.5 mmol/L; 95% CI, -20.7 to -16.3; P < 0.001), and these reductions were sustained through the study period. There were no significant changes in hospitalization rate for pulmonary exacerbations and Pseudomonas aeruginosa infection status with treatment.Conclusions: In this real-world multicenter cohort of children and adults, LUM/IVA treatment was associated with significant improvements in growth and reductions in sweat chloride without statistically significant or clinically meaningful changes in lung function, hospitalization rates, or P. aeruginosa infection.Clinical trial registered with www.clinicaltrials.gov (NCT02477319).
Keywords: clinical effectiveness; cystic fibrosis; ivacaftor; lumacaftor; postapproval study.
Figures
Comment in
-
The PROSPECT Is Bright for CFTR Modulators.Ann Am Thorac Soc. 2021 Jan;18(1):32-33. doi: 10.1513/AnnalsATS.202007-881ED. Ann Am Thorac Soc. 2021. PMID: 33385230 Free PMC article. No abstract available.
References
-
- Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzelczak Z, et al. Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA. Science. 1989;245:1066–1073. [Published erratum appears in Science 245:1437.] - PubMed
-
- Kerem B, Rommens JM, Buchanan JA, Markiewicz D, Cox TK, Chakravarti A, et al. Identification of the cystic fibrosis gene: genetic analysis. Science. 1989;245:1073–1080. - PubMed
-
- Rowe SM, Miller S, Sorscher EJ. Cystic fibrosis. N Engl J Med. 2005;352:1992–2001. - PubMed
-
- Cystic Fibrosis Foundation. Bethesda, MD: Cystic Fibrosis Foundation; 2018. Patient registry 2018 annual data report.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
