

Prospective randomised controlled trial using the REthinking Clinical Trials (REaCT) platform and National Surgical Quality Improvement Program (NSQIP) to compare no preparation versus preoperative oral antibiotics alone for surgical site infection rates in elective colon surgery: a protocol
- PMID: 32647023
- PMCID: PMC7351286
- DOI: 10.1136/bmjopen-2020-036866
Prospective randomised controlled trial using the REthinking Clinical Trials (REaCT) platform and National Surgical Quality Improvement Program (NSQIP) to compare no preparation versus preoperative oral antibiotics alone for surgical site infection rates in elective colon surgery: a protocol
Abstract
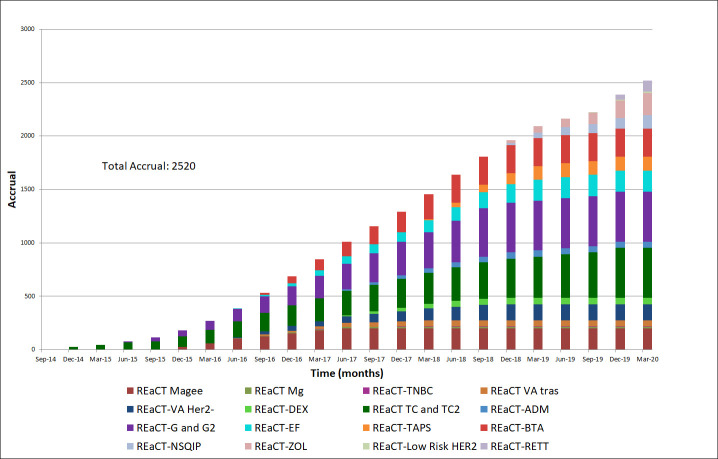
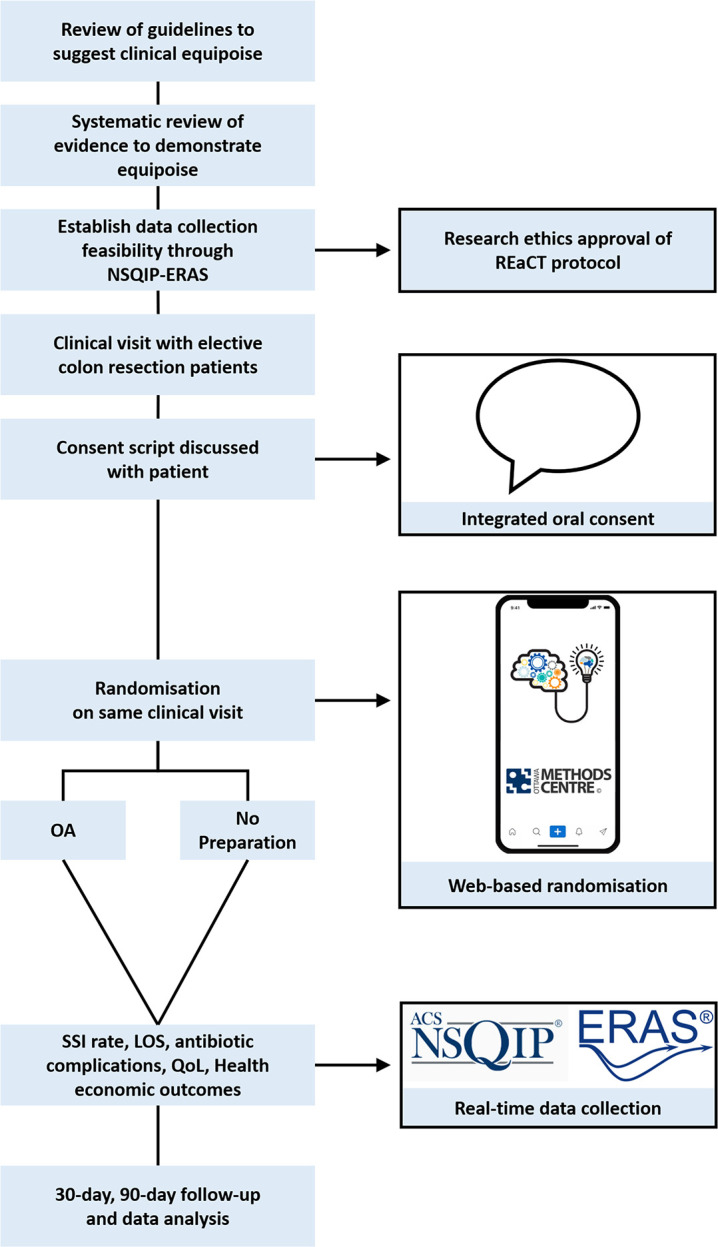
Introduction: Despite 40 randomised controlled trials (RCTs) investigating preoperative oral antibiotics (OA) and mechanical bowel preparation (MBP) to reduce surgical site infection (SSI) rate following colon surgery, there has never been an RCT published comparing OA alone versus no preparation. Of the four possible regimens (OA alone, MBP alone, OA plus MBP and no preparation), randomised evidence is conflicting for studied groups. Furthermore, guidelines vary, with recommendations for OA alone, OA plus MBP or no preparation. The National Surgical Quality Improvement Program (NSQIP) has automated data collection for surgical patients. Similarly, the 'REthinking Clinical Trials' (REaCT) platform increases RCT enrolment by simplifying pragmatic trial design. In this novel RCT protocol, we combine REaCT and NSQIP to compare OA alone versus no preparation for SSI rate reduction in elective colon surgery. To our knowledge, this is the first published RCT protocol that leverages NSQIP for data collection. In our feasibility study, 67 of 74 eligible patients (90%) were enrolled and 63 of 67 (94%) were adherent to protocol. The 'REaCT-NSQIP' trial design has great potential to efficiently generate level I evidence for other perioperative interventions.
Methods and analysis: SSI rates following elective colorectal surgery after preoperative OA or no preparation will be compared. We predict 45% relative rate reduction of SSI, improvement in length of stay, reduced costs and increased quality of life, with similar antibiotic-related complications. Consent, using the 'integrated consent model', and randomisation on a mobile device are completed by the surgeon in a single clinical encounter. Data collection for the primary end point is automatic through NSQIP. Analysis of cost per weighted case, cost utility and quality-adjusted life years will be done.
Ethics and dissemination: This study is approved by The Ontario Cancer Research Ethics Board. Results will be disseminated in surgical conferences and peer-reviewed journals.
Trial registration number: NCT03663504; Pre-results, recruitment phase.
Keywords: clinical trials; colorectal surgery; infection control; statistics & research methods; wound management.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: RCA, SSA, HM, AJ, KS and KT do not have any conflicts of interests to disclose. DAF is a senior scientist at Ottawa Methods Centre. DAF and MC are the founders and leads of the Ottawa REaCT study platform.
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous