

An exploratory cross-sectional study of subclinical vascular damage in patients with polymyalgia rheumatica
- PMID: 32647217
- PMCID: PMC7347873
- DOI: 10.1038/s41598-020-68215-8
An exploratory cross-sectional study of subclinical vascular damage in patients with polymyalgia rheumatica
Abstract
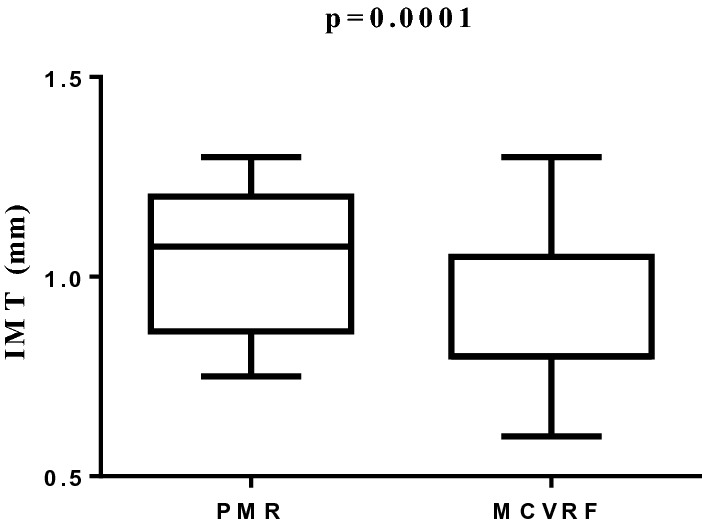
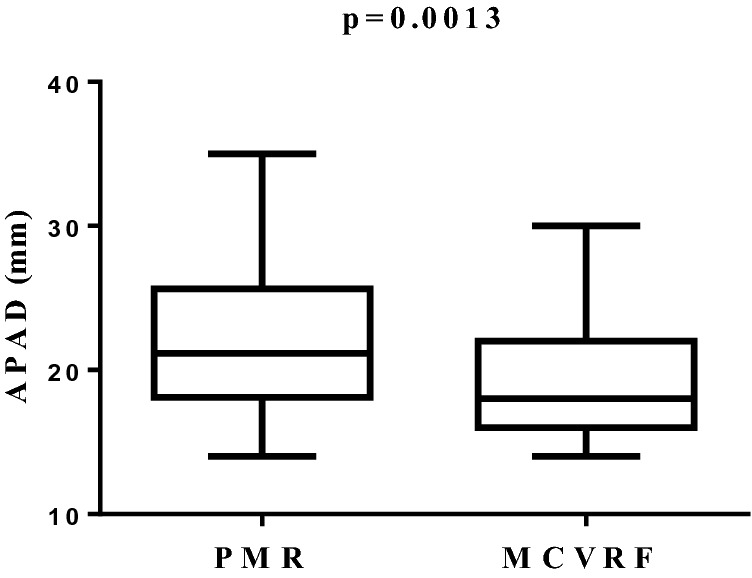
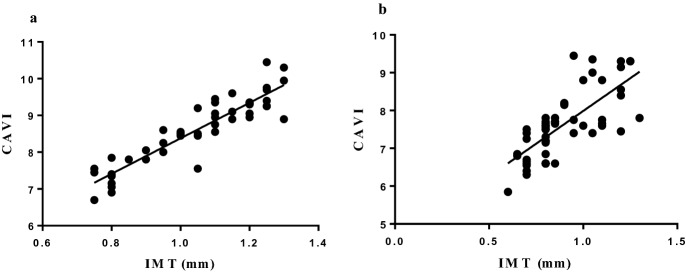
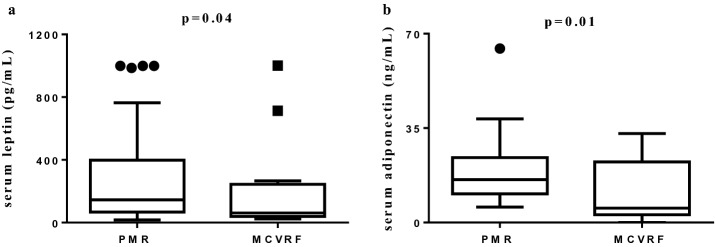
The aim of the study was to investigate the presence of subclinical vascular damage in polymyalgia rheumatica (PMR). We enrolled PMR patients having major cardiovascular risk factors (MCVRF) and, as controls, patients with MCVRF. All underwent: color Doppler ultrasound to evaluate the common carotid intima-media thickness (IMT), the anterior-posterior abdominal aortic diameter (APAD), and the prevalence of carotid artery stenosis; the cardio-ankle vascular index (CAVI) to measure arterial stiffness together with the ankle-brachial index (ABI) to investigate the presence of lower-extremity peripheral arterial disease. Finally, we measured the serum levels of adipocytokines implicated in vascular dysfunction. As a result, 48 PMR and 56 MCVRF patients were included. An increase of IMT (1.07/0.8-1.2 vs 0.8/0.8-1.05; p = 0.0001), CAVI (8.7/7.8-9.3 vs 7.6/6.9-7.8; p < 0.0001) and APAD values (21.15/18.1-25.6 vs 18/16-22; p = 0.0013) was found in PMR patients with respect to controls. No differences were reported in the prevalence of carotid artery stenosis or ABI values between the two groups. A significant correlation between IMT and CAVI in PMR and MCVRF subjects (r2 = 0.845 and r2 = 0.556, respectively; p < 0.01) was found. Leptin levels (pg/mL; median/25th-75th percentile) were higher in PMR than in MCVRF subjects (145.1/67-398.6 vs 59.5/39.3-194.3; p = 0.04). Serum levels of adiponectin (ng/mL) were higher in PMR patients (15.9/10.65-24.1 vs 6.1/2.8-22.7; p = 0.01), while no difference in serum levels of resistin (ng/mL) was found between PMR and MCVRF subjects (0.37/0.16-0.66 vs 0.26/0.14-1.24). Our study shows an increased subclinical vascular damage in PMR patients compared to those with MCVRF, paving the way for further studies aimed at planning primary cardiovascular prevention in this population.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bremander A, et al. Population-based estimates of common comorbidities and cardiovascular disease in ankylosing spondylitis. Arthritis Care Res. (Hoboken) 2011;63:550–556. - PubMed
-
- Essers I, et al. Ankylosing spondylitis and risk of ischaemic heart disease: A population-based cohort study. Ann. Rheum. Dis. 2016;75:203–209. - PubMed
-
- Haroon NN, et al. Patients with ankylosing spondylitis have increased cardiovascular and cerebrovascular mortality: A population-based study. Ann. Intern. Med. 2015;163:409–416. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
