

The intraprostatic immune environment after stereotactic body radiotherapy is dominated by myeloid cells
- PMID: 32647353
- PMCID: PMC7794088
- DOI: 10.1038/s41391-020-0249-8
The intraprostatic immune environment after stereotactic body radiotherapy is dominated by myeloid cells
Abstract
Background: Hundreds of ongoing clinical trials combine radiation therapy, mostly delivered as stereotactic body radiotherapy (SBRT), with immune checkpoint blockade. However, our understanding of the effect of radiotherapy on the intratumoral immune balance is inadequate, hindering the optimal design of trials that combine radiation therapy with immunotherapy. Our objective was to characterize the intratumoral immune balance of the malignant prostate after SBRT in patients.
Methods: Sixteen patients with high-risk, non-metastatic prostate cancer at comparable Gleason Grade disease underwent radical prostatectomy with (n = 9) or without (n = 7) neoadjuvant SBRT delivered in three fractions of 8 Gy over 5 days completed 2 weeks before surgery. Freshly resected prostate specimens were processed to obtain single-cell suspensions, and immune-phenotyped for major lymphoid and myeloid cell subsets by staining with two separate 14-antibody panels and multicolor flow cytometry analysis.
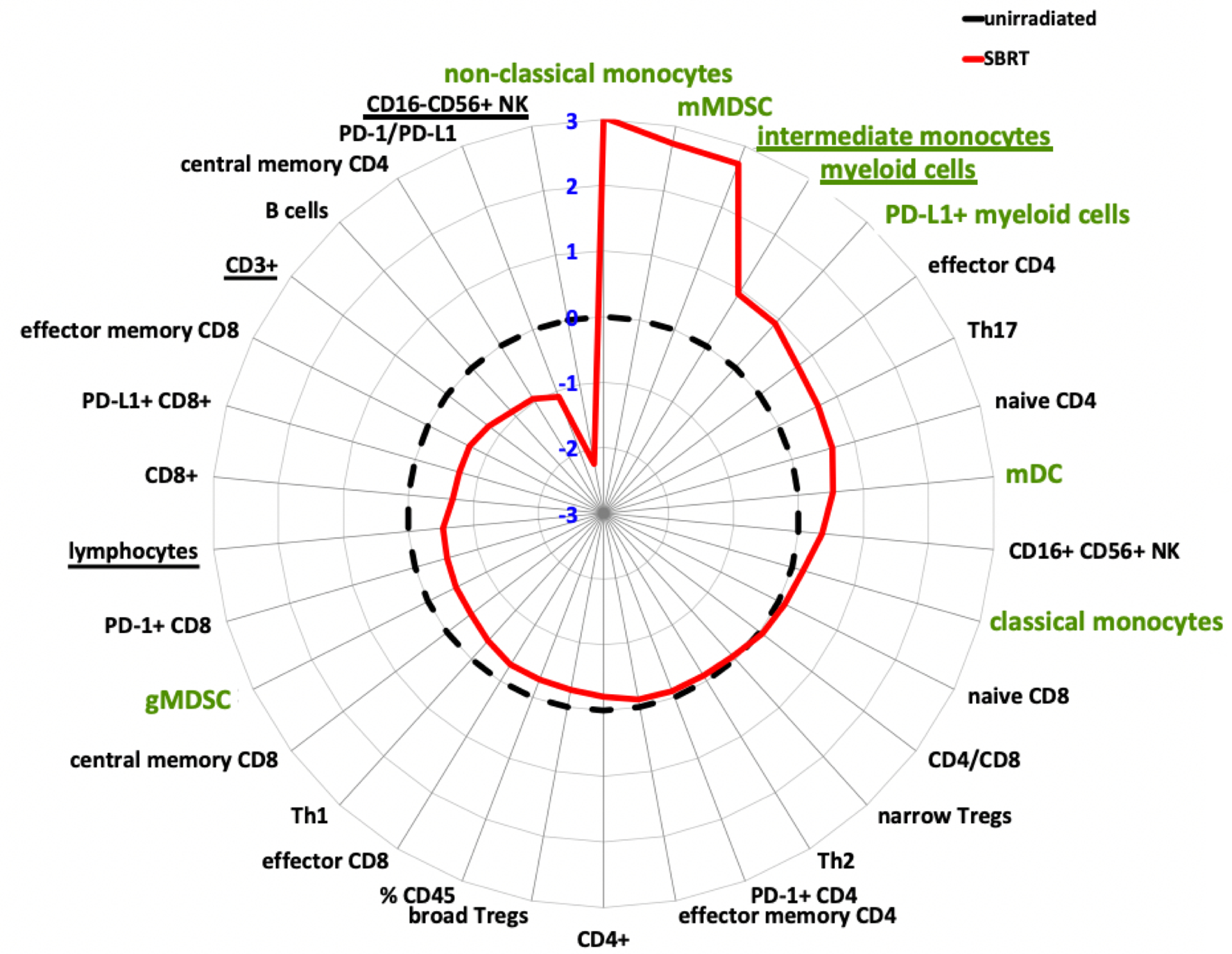
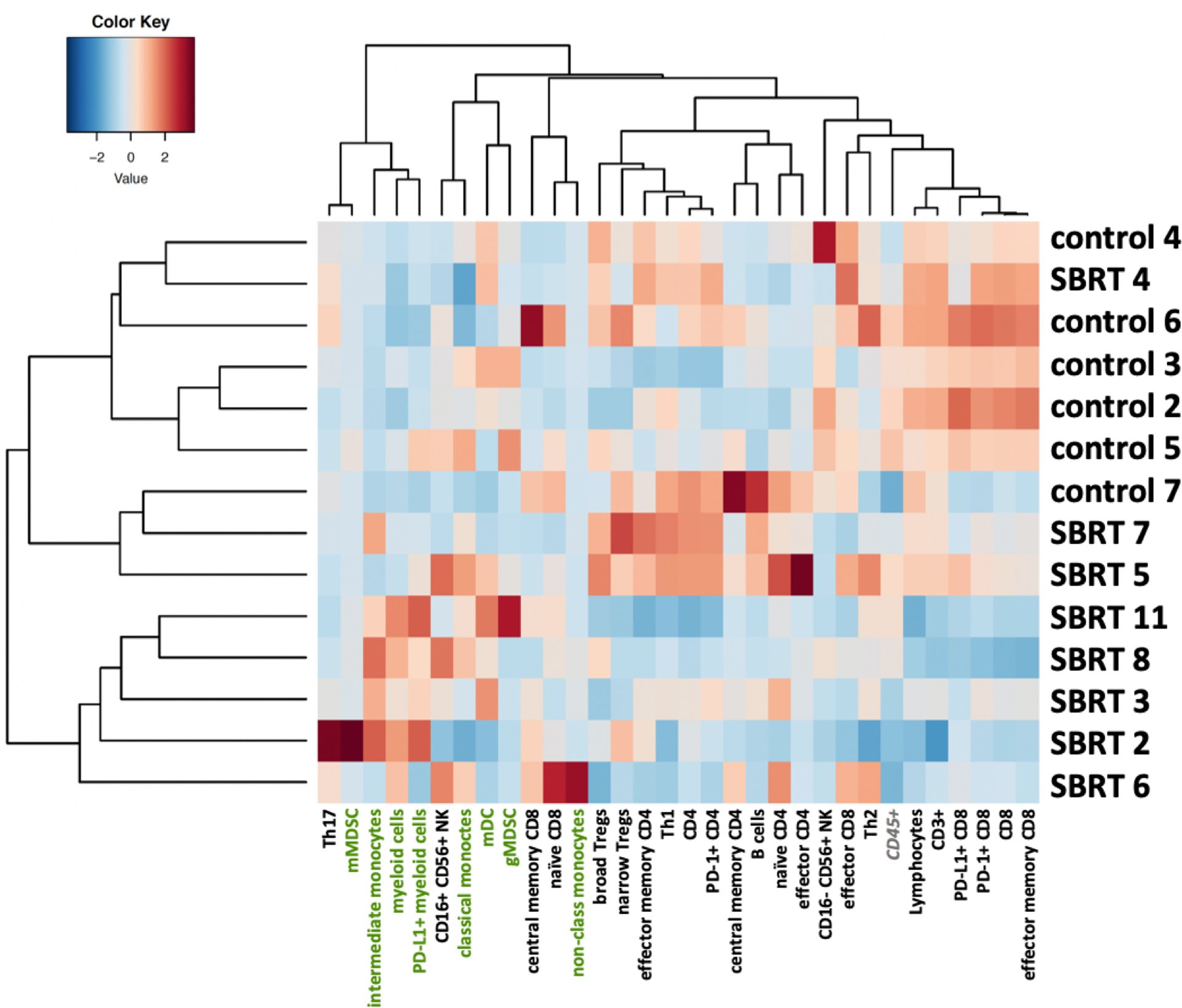
Results: Malignant prostates 2 weeks after SBRT had an immune infiltrate dominated by myeloid cells, whereas malignant prostates without preoperative treatment were more lymphoid-biased (myeloid CD45+ cells 48.4 ± 19.7% vs. 25.4 ± 7.0%; adjusted p-value = 0.11; and CD45+ lymphocytes 51.6 ± 19.7% vs. 74.5 ± 7.0%; p = 0.11; CD3+ T cells 35.2 ± 23.8% vs. 60.9 ± 9.7%; p = 0.12; mean ± SD).
Conclusion: SBRT drives a significant lymphoid to myeloid shift in the prostate-tumor immune infiltrate. This may be of interest when combining SBRT with immunotherapies, particularly in prostate cancer.
Conflict of interest statement
DISCLOSURE OF POTENTIAL CONFLICT OF INTEREST
The authors declare no competing financial interests, activities, relationships, or affiliations related to this manuscript.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
