

Dissecting and rebuilding the glioblastoma microenvironment with engineered materials
- PMID: 32647587
- PMCID: PMC7347297
- DOI: 10.1038/s41578-019-0135-y
Dissecting and rebuilding the glioblastoma microenvironment with engineered materials
Abstract
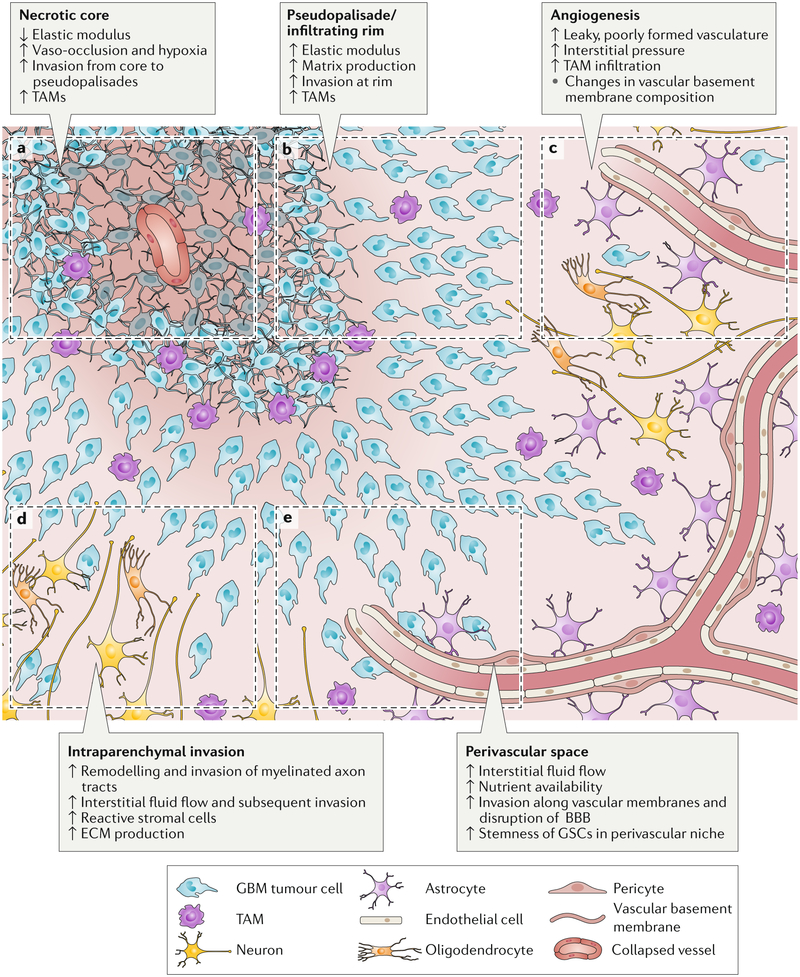
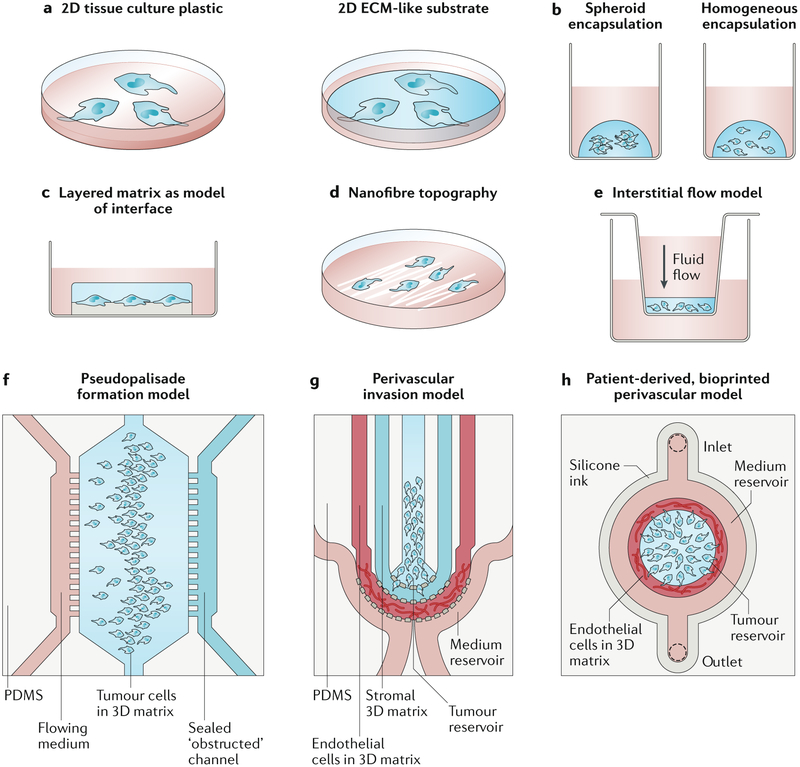
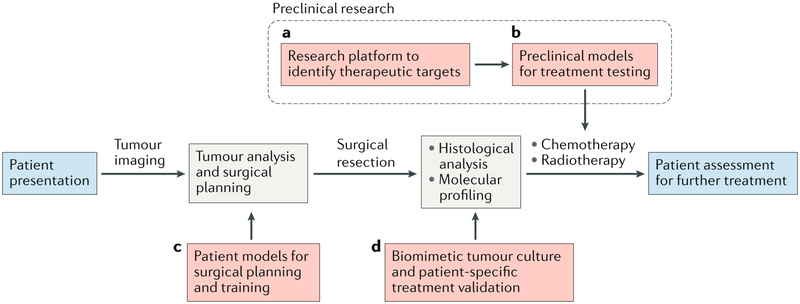
Glioblastoma (GBM) is the most aggressive and common form of primary brain cancer. Several decades of research have provided great insight into GBM progression; however, the prognosis remains poor with a median patient survival time of ~ 15 months. The tumour microenvironment (TME) of GBM plays a crucial role in mediating tumour progression and thus is being explored as a therapeutic target. Progress in the development of treatments targeting the TME is currently limited by a lack of model systems that can accurately recreate the distinct extracellular matrix composition and anatomic features of the brain, such as the blood-brain barrier and axonal tracts. Biomaterials can be applied to develop synthetic models of the GBM TME to mimic physiological and pathophysiological features of the brain, including cellular and ECM composition, mechanical properties, and topography. In this Review, we summarize key features of the GBM microenvironment and discuss different strategies for the engineering of GBM TME models, including 2D and 3D models featuring chemical and mechanical gradients, interfaces and fluid flow. Finally, we highlight the potential of engineered TME models as platforms for mechanistic discovery and drug screening as well as preclinical testing and precision medicine.
Conflict of interest statement
Competing Interest Statements: The authors declare no competing financial interests.
Figures
References
-
- Stupp R et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet. Oncol 10, 459–66 (2009). - PubMed
-
- Watanabe M, Tanaka R & Takeda N Magnetic resonance imaging and histopathology of cerebral gliomas. Neuroradiology 34, 463–469 (1992). - PubMed