

Optimal target in septic shock resuscitation
- PMID: 32647714
- PMCID: PMC7333135
- DOI: 10.21037/atm-20-1120
Optimal target in septic shock resuscitation
Abstract
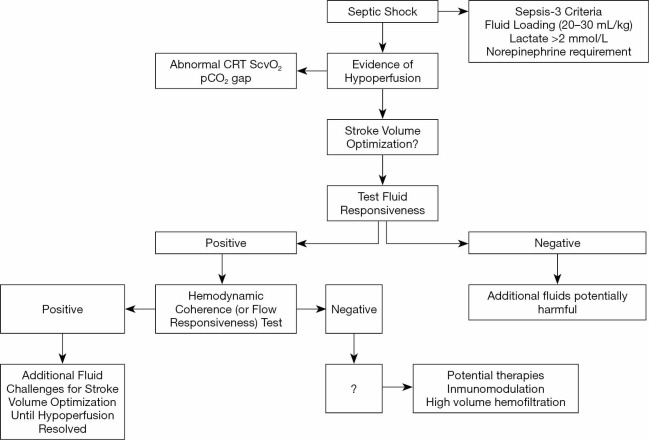
Septic shock presents a high risk of morbidity and mortality. Through therapeutic strategies, such as fluid administration and vasoactive agents, clinicians intend to rapidly restore tissue perfusion. Nonetheless, these interventions have narrow therapeutic margins. Adequate perfusion monitoring is paramount to avoid progressive hypoperfusion or detrimental over-resuscitation. During early stages of septic shock, macrohemodynamic derangements, such as hypovolemia and decreased cardiac output (CO) tend to predominate. However, during late septic shock, endothelial and coagulation dysfunction induce severe alterations of the microcirculation, making it more difficult to achieve tissue reperfusion. Multiple perfusion variables have been described in the literature, from bedside clinical examination to complex laboratory tests. Moreover, all of them present inherent flaws and limitations. After the ANDROMEDA-SHOCK trial, there is evidence that capillary refill time (CRT) is an interesting resuscitation target, due to its rapid kinetics and correlation with deep hypoperfusion markers. New concepts such as hemodynamic coherence and flow responsiveness may be used at the bedside to select the best treatment strategies at any time-point. A multimodal perfusion monitoring and an integrated analysis with macrohemodynamic parameters is mandatory to optimize the resuscitation of septic shock patients.
Keywords: Septic shock; capillary refill time (CRT); fluid therapy; lactate; microcirculation; resuscitation.
2020 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/atm-20-1120). The series “Hemodynamic monitoring in critically ill patients” was commissioned by the editorial office without any funding or sponsorship. GH served as the unpaid Guest Editor of the series. The other authors have no other conflicts of interest to declare.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials