

Understanding ventriculo-arterial coupling
- PMID: 32647720
- PMCID: PMC7333110
- DOI: 10.21037/atm.2020.04.10
Understanding ventriculo-arterial coupling
Abstract
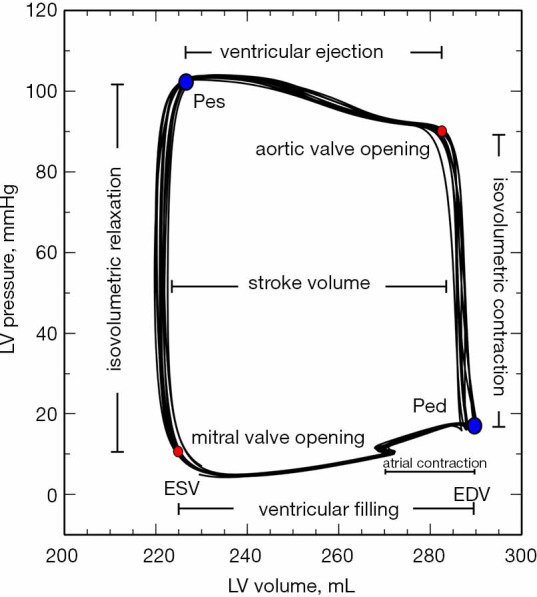
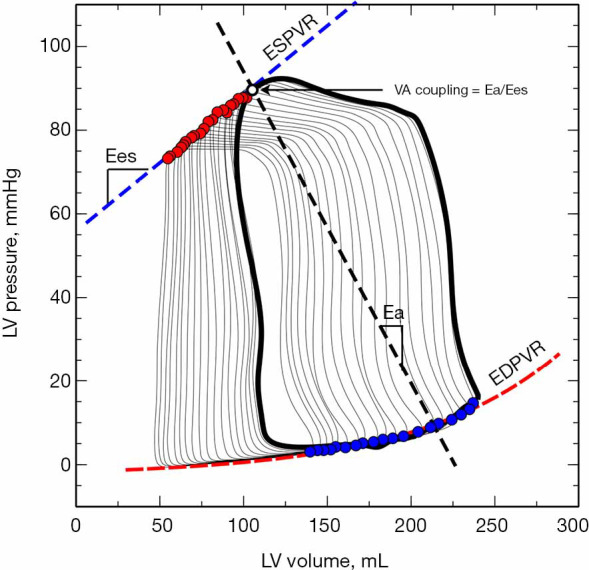
In the late 19th century, Otto Frank published the first description of a ventricular pressure-volume diagram, thus laid the foundation for modern cardiovascular physiology. Since then, the analysis of the pressure-volume loops became a reference tool for the study of the ventricular pump properties. However, understanding cardiovascular performance requires both the evaluation of ventricular properties and the modulating effects of the arterial system, since the heart and the arterial tree are anatomically and functionally related structures. The study of the coupling between the cardiac function and the properties of the arterial system, or ventriculo-arterial (VA) coupling, provides then a comprehensive characterization of the performance of the cardiovascular system in both health and disease. The assessment of cardiovascular function is an essential element of the hemodynamic evaluation of critically ill patients. Both left and right ventricular dysfunction and arterial system disturbances are frequent in these patients. Since VA coupling ultimately defines de performance and efficiency of the cardiovascular system, the analysis of the interaction between the heart and the arterial system could offer a broader perspective of the hemodynamic disorders associated with common conditions, such as septic shock, heart failure, or right ventricular dysfunction. Moreover, this analysis could also provide valuable information about their pathophysiological mechanisms and may help to determine the best therapeutic strategy to correct them. In this review, we will describe the basic principles of the VA coupling assessment, its limitations, and the most common methods for its estimation at the bedside. Then, we will summarize the current knowledge of the application of VA coupling in critically ill patients and suggest some recommendations for further research.
Keywords: Ventricular-arterial coupling; arterial effective elastance; critical care; pressure-volume loop; ventricular elastance.
2020 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/atm.2020.04.10). The series “Hemodynamic Monitoring in Critically Ill Patients” was commissioned by the editorial office without any funding or sponsorship. MIMG reports personal fees from Edwards Lifesciencies, outside the submitted work. AS has no other conflicts to disclose.
Figures
References
-
- Yin FCP, Avolio AP. Ventricular/vascular coupling: clinical, physiological, and engineering aspects. New York: Springer-Verlag; 1987.
Publication types
LinkOut - more resources
Full Text Sources
Medical