

Final Results of a Phase I/II Trial of the Combination Bendamustine and Rituximab With Temsirolimus (BeRT) in Relapsed Mantle Cell Lymphoma and Follicular Lymphoma
- PMID: 32647802
- PMCID: PMC7306311
- DOI: 10.1097/HS9.0000000000000398
Final Results of a Phase I/II Trial of the Combination Bendamustine and Rituximab With Temsirolimus (BeRT) in Relapsed Mantle Cell Lymphoma and Follicular Lymphoma
Abstract
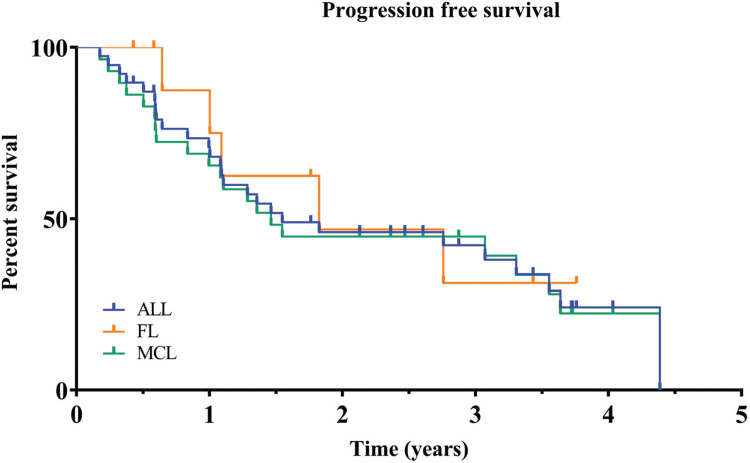
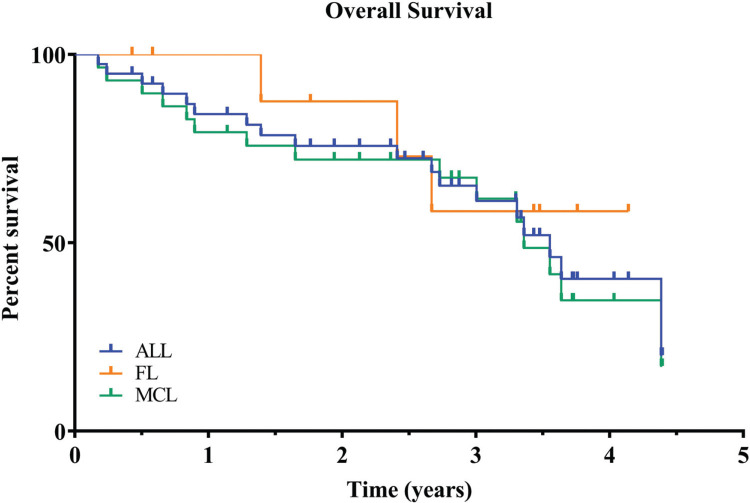
In this phase I/II study, we explored the combination of Temsirolimus with Bendamustine and Rituximab (BeRT) in patients with relapsed or refractory (r/r) follicular lymphoma (FL) or mantle cell lymphoma (MCL). Patients with 1 to 3 previous therapies received Bendamustine (90 mg/m2, day 1 + 2) and Rituximab (375 mg/m2, day 1) with Temsirolimus in doses from 25 to 75 mg in phase I and 50 mg Temsirolimus in phase II, added on day 1, 8, 15 of a 28 days cycle. The primary endpoint of the phase II was ORR at the end of treatment. Overall, 39 (29 MCL, 10 FL) patients were included. Median age was 71 years and median pretreatment number was 2. Grade 3/4 non-hematologic adverse events were rare and included hyperglycemia in 3 patients (7%) and angioedema in 2 patients (5%). Infectious complications grade 3/4 were observed in 9 patients (23%). Hematologic grade 3/4 events included leukopenia in 22 (56%), neutropenia in 18 (46%), lymphopenia in 16 (41%) and thrombocytopenia in 14 patients (36%). An objective response (best response) was observed in 33/39 patients (89%; 24 MCL (89%) and 9 FL (90%)), including 14 CR (38%; 12 MCL (36%) and 2 FL (20%)). Median PFS is 1.5y for MCL and 1.82 years for FL, and median OS has not been reached for either entity. This data demonstrates promising efficacy of Temsirolimus in r/r MCL and FL with acceptable toxicity. The BeRT regimen may be used as a treatment option for both entities.
Copyright © 2020 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Conflict of interest statement
Conflicts of interest: JA: Pfizer, Roche: Honoraria.
Figures
References
-
- Buske C, Hoster E, Dreyling M, et al. The addition of rituximab to front-line therapy with CHOP (R-CHOP) results in a higher response rate and longer time to treatment failure in patients with lymphoplasmacytic lymphoma: results of a randomized trial of the German Low-Grade Lymphoma Study Group (GLSG). Leukemia. 2009;23:153–161. - PubMed
-
- Kluin-Nelemans HC, Hoster E, Hermine O, et al. Treatment of older patients with mantle-cell lymphoma. N Engl J Med. 2012;367:520–531. - PubMed
-
- Dreyling M, Ghielmini M, Rule S, et al. Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28:59–62. - PubMed
-
- Hidalgo M, Buckner JC, Erlichman C, et al. A phase I and pharmacokinetic study of temsirolimus (CCI-779) administered intravenously daily for 5 days every 2 weeks to patients with advanced cancer. Clin Cancer Res. 2006;12:5755–5763. - PubMed
LinkOut - more resources
Full Text Sources