

Cardiovascular morbidity and mortality among persons diagnosed with tuberculosis: A systematic review and meta-analysis
- PMID: 32649721
- PMCID: PMC7351210
- DOI: 10.1371/journal.pone.0235821
Cardiovascular morbidity and mortality among persons diagnosed with tuberculosis: A systematic review and meta-analysis
Abstract
Introduction: The emerging epidemiological evidence of increased cardiovascular disease (CVD) risk among persons diagnosed with tuberculosis (TB) has not been systematically reviewed to date. Our aim was to review the existing epidemiological evidence for elevated risk of CVD morbidity and mortality among persons diagnosed with TB compared to controls.
Materials and methods: EMBASE, MEDLINE, and Cochrane databases were searched (inception to January 2020) for terms related to "tuberculosis" and "cardiovascular diseases". Inclusion criteria: trial, cohort, or case-control study design; patient population included persons diagnosed with TB infection or disease; relative risk (RR) estimate and confidence interval reported for CVD morbidity or mortality compared to suitable controls. Exclusion criteria: no TB or CVD outcome definition; duplicate study; non-English abstract; non-human participants. Two reviewers screened studies, applied ROBINS-I tool to assess risk of bias, and extracted data independently. Random effects meta-analysis estimated a pooled RR of CVD morbidity and mortality for persons diagnosed with TB compared to controls.
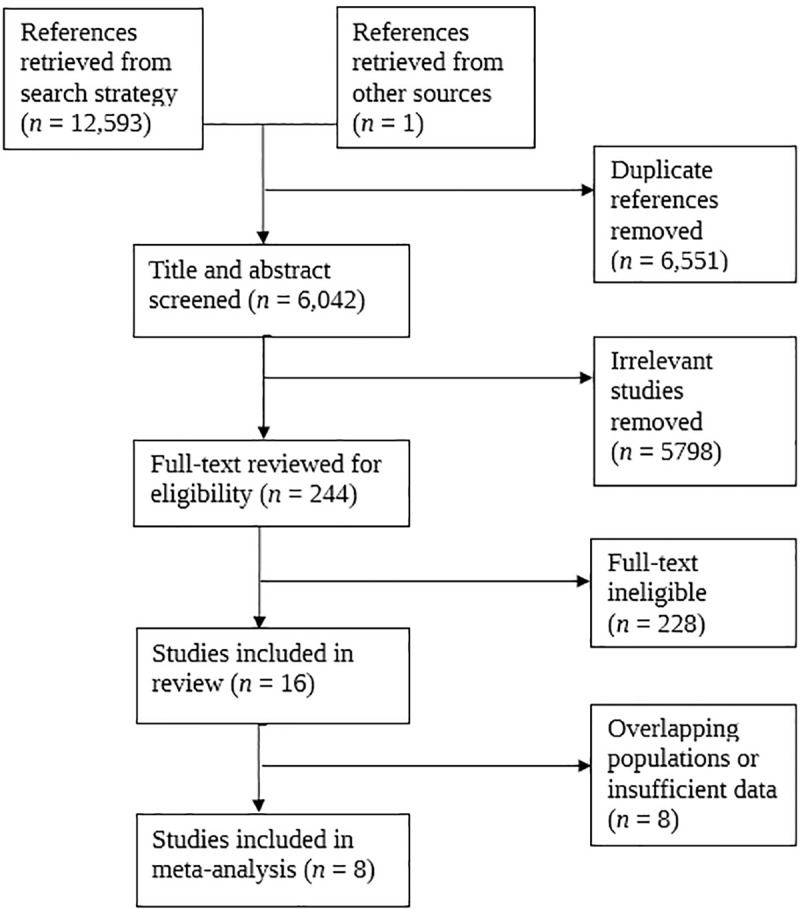
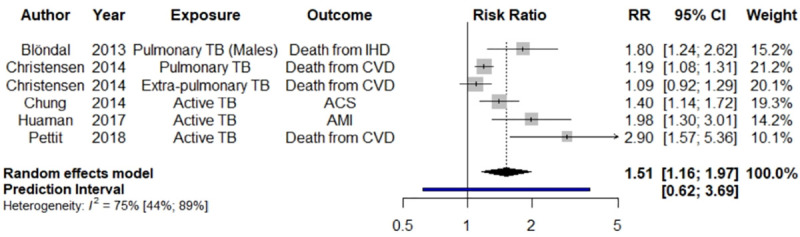
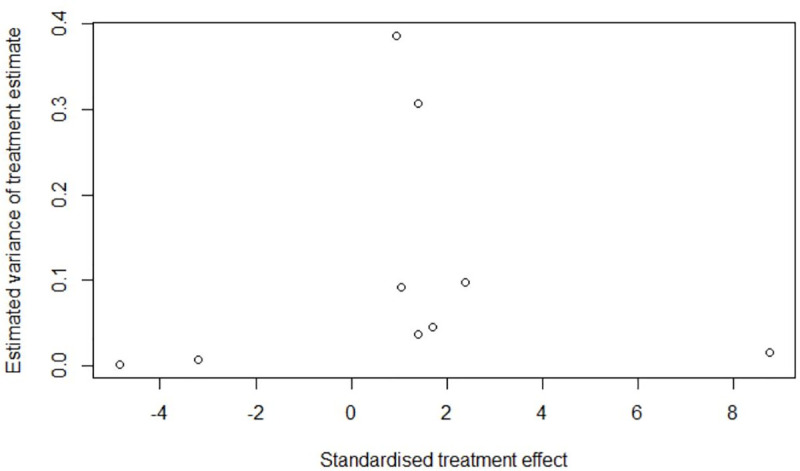
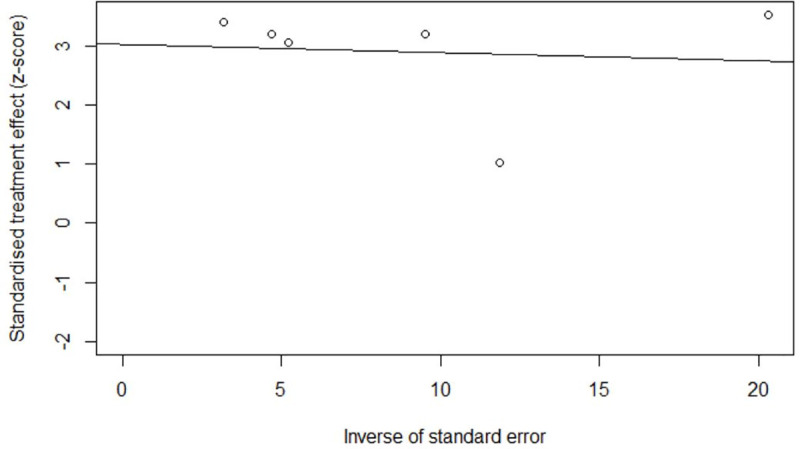
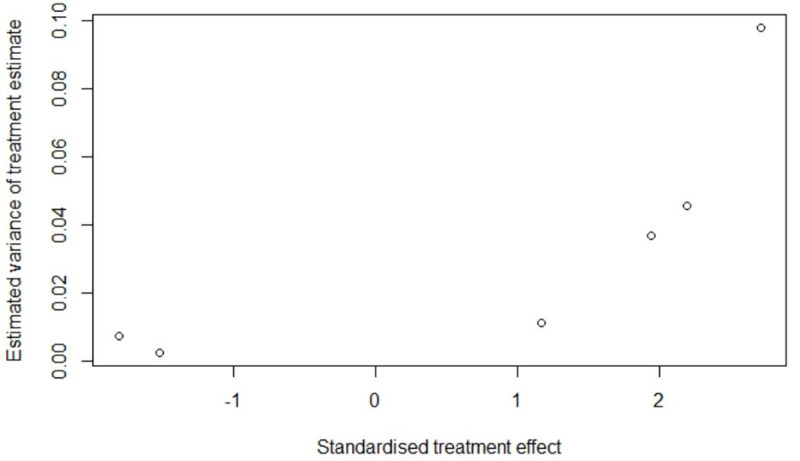
Results: 6,042 articles were identified, 244 full texts were reviewed, and 16 were included, meta-analyzing subsets of 8 studies' RR estimates. We estimated a pooled RR of 1.51 (95% CI: 1.16-1.97) for major adverse cardiac events among those diagnosed with TB compared to non-TB controls (p = 0.0024). A 'serious' pooled risk of bias was found across studies with between-study heterogeneity (I2 = 75.3%).
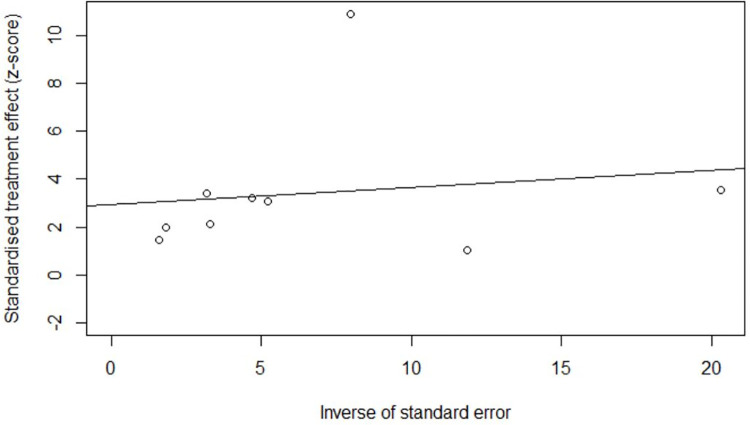
Conclusions: TB appears to be a marker for increased CVD risk; however, the literature is limited and is accompanied by serious risk of confounding bias and evidence of publication bias. Further retrospective and prospective studies are needed. Pending this evidence, best practice may be to consider persons diagnosed with TB at higher risk of CVD as a precautionary measure.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization (WHO). Global Tuberculosis Report 2018. Geneva, Switzerland: World Health Organization; 2018. Available: https://www.who.int/tb/publications/global_report/en/
-
- World Health Organization (WHO). Global Tuberculosis Report 2019. Geneva, Switzerland: World Health Organization; 2019. Available: https://www.who.int/tb/publications/global_report/en/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
