

Interstitial lung abnormalities detected incidentally on CT: a Position Paper from the Fleischner Society
- PMID: 32649920
- PMCID: PMC7970441
- DOI: 10.1016/S2213-2600(20)30168-5
Interstitial lung abnormalities detected incidentally on CT: a Position Paper from the Fleischner Society
Abstract
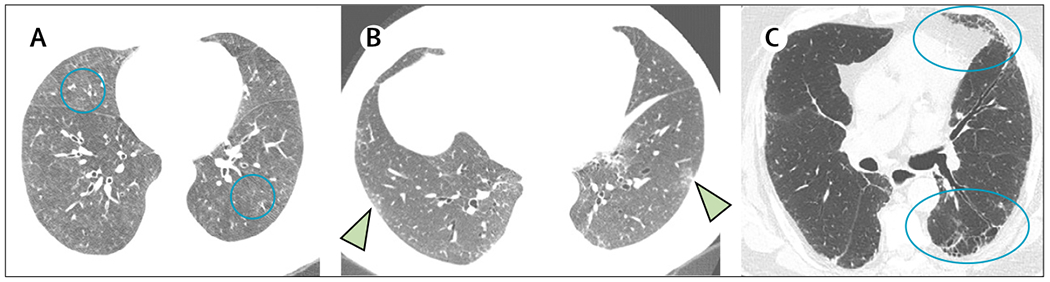
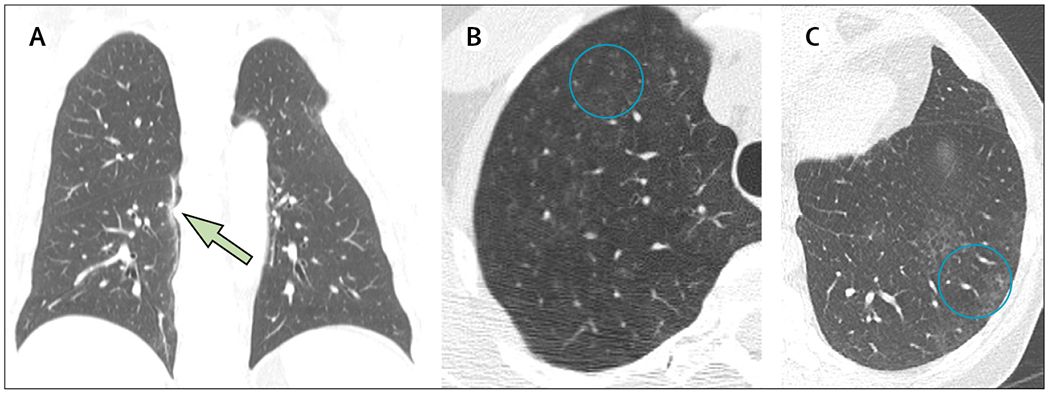
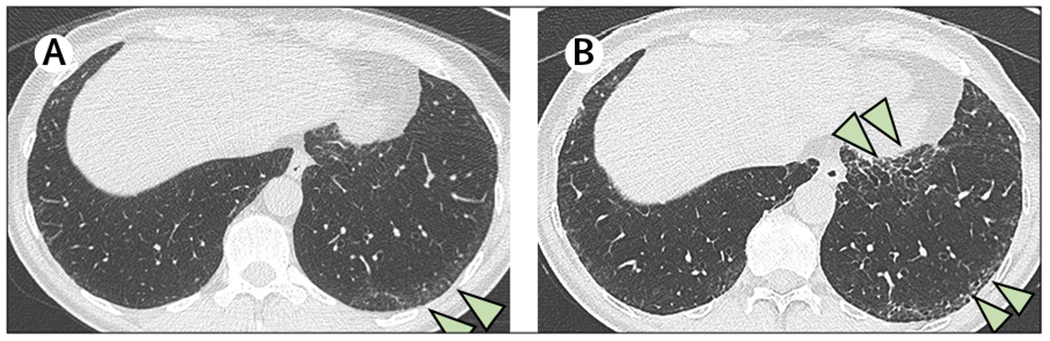
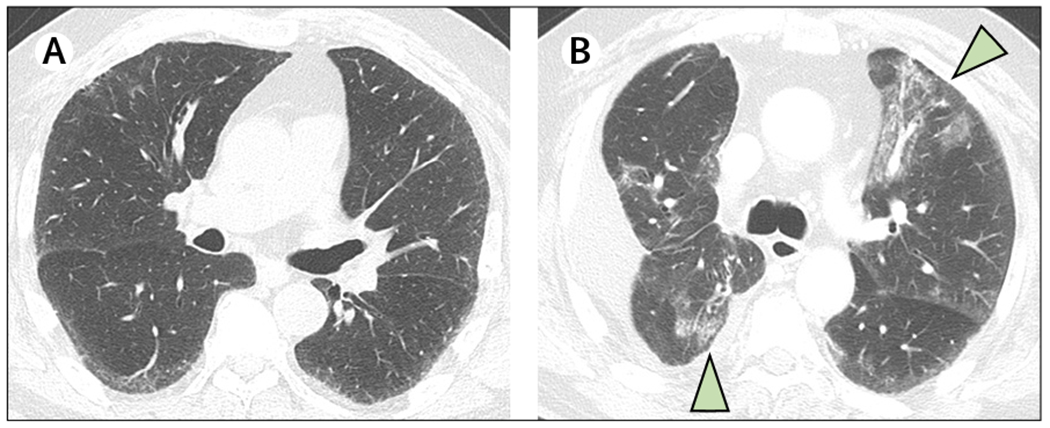
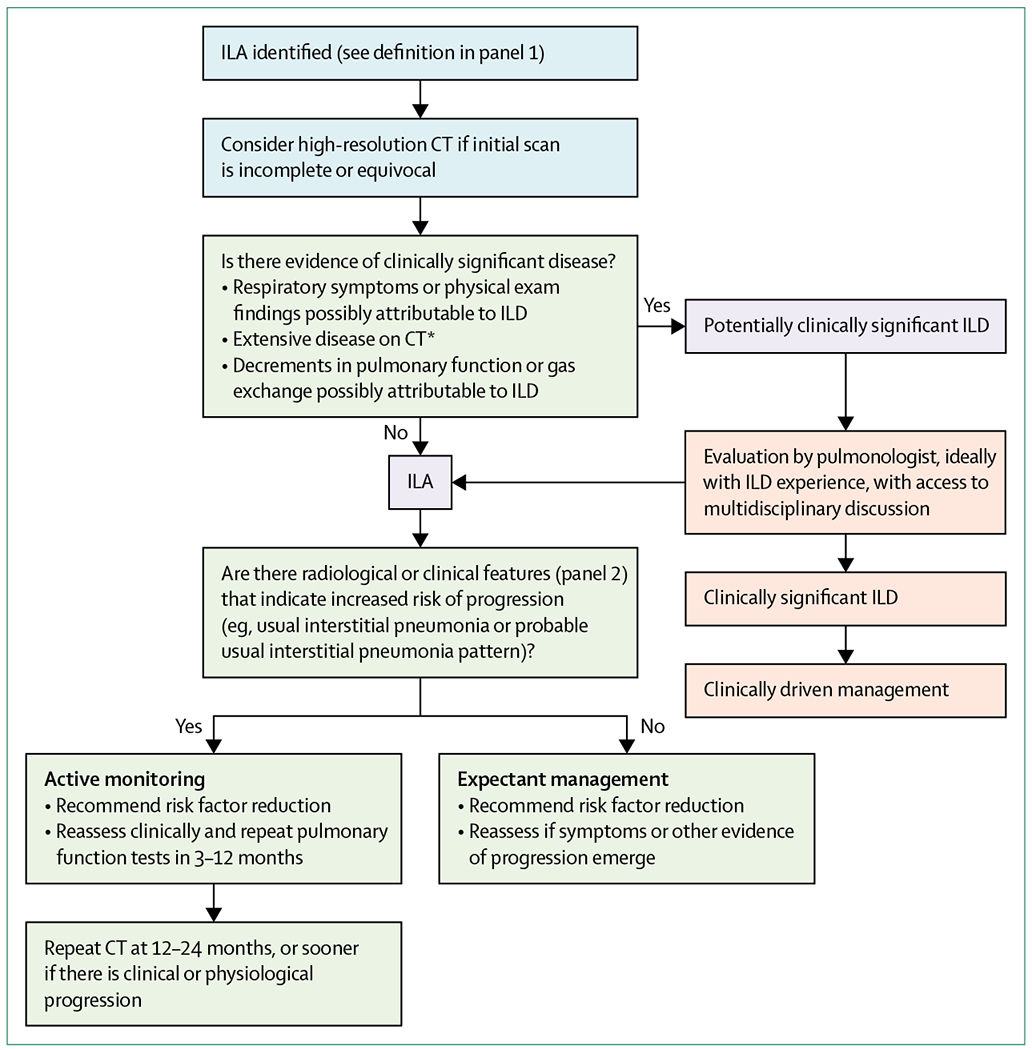
The term interstitial lung abnormalities refers to specific CT findings that are potentially compatible with interstitial lung disease in patients without clinical suspicion of the disease. Interstitial lung abnormalities are increasingly recognised as a common feature on CT of the lung in older individuals, occurring in 4-9% of smokers and 2-7% of non-smokers. Identification of interstitial lung abnormalities will increase with implementation of lung cancer screening, along with increased use of CT for other diagnostic purposes. These abnormalities are associated with radiological progression, increased mortality, and the risk of complications from medical interventions, such as chemotherapy and surgery. Management requires distinguishing interstitial lung abnormalities that represent clinically significant interstitial lung disease from those that are subclinical. In particular, it is important to identify the subpleural fibrotic subtype, which is more likely to progress and to be associated with mortality. This multidisciplinary Position Paper by the Fleischner Society addresses important issues regarding interstitial lung abnormalities, including standardisation of the definition and terminology; predisposing risk factors; clinical outcomes; options for initial evaluation, monitoring, and management; the role of quantitative evaluation; and future research needs.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
References
-
- Schwarz MI, King TE Jr. Interstitial lung disease, 5th edn. Shelton, CT: People’s Medical Publishing House, 2011.
-
- Hatabu H, Hunninghake GM, Lynch DA. Interstitial lung abnormality: recognition and perspectives. Radiology 2019; 291: 1–3. - PubMed
