

Repeated 5-day cycles of low dose aldesleukin in amyotrophic lateral sclerosis (IMODALS): A phase 2a randomised, double-blind, placebo-controlled trial
- PMID: 32651161
- PMCID: PMC7502670
- DOI: 10.1016/j.ebiom.2020.102844
Repeated 5-day cycles of low dose aldesleukin in amyotrophic lateral sclerosis (IMODALS): A phase 2a randomised, double-blind, placebo-controlled trial
Abstract
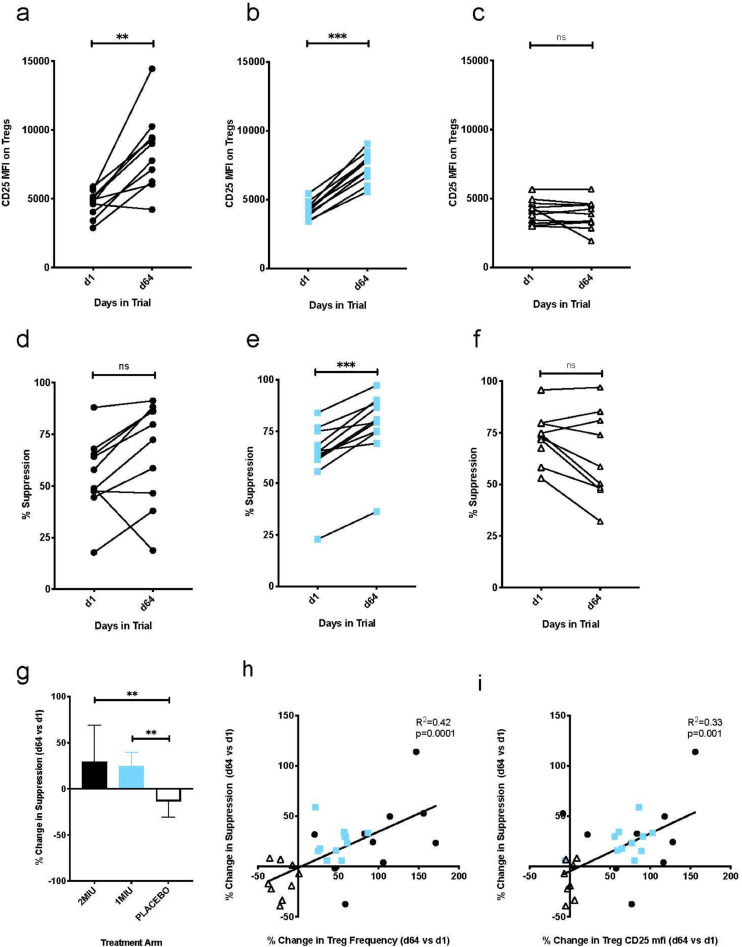
Background: Low-dose interleukin-2 (ld-IL-2) enhances regulatory T-cell (Treg) function in auto-inflammatory conditions. Neuroinflammation being a pathogenic feature of amyotrophic lateral sclerosis (ALS), we evaluated the pharmacodynamics and safety of ld-IL-2 in ALS subjects.
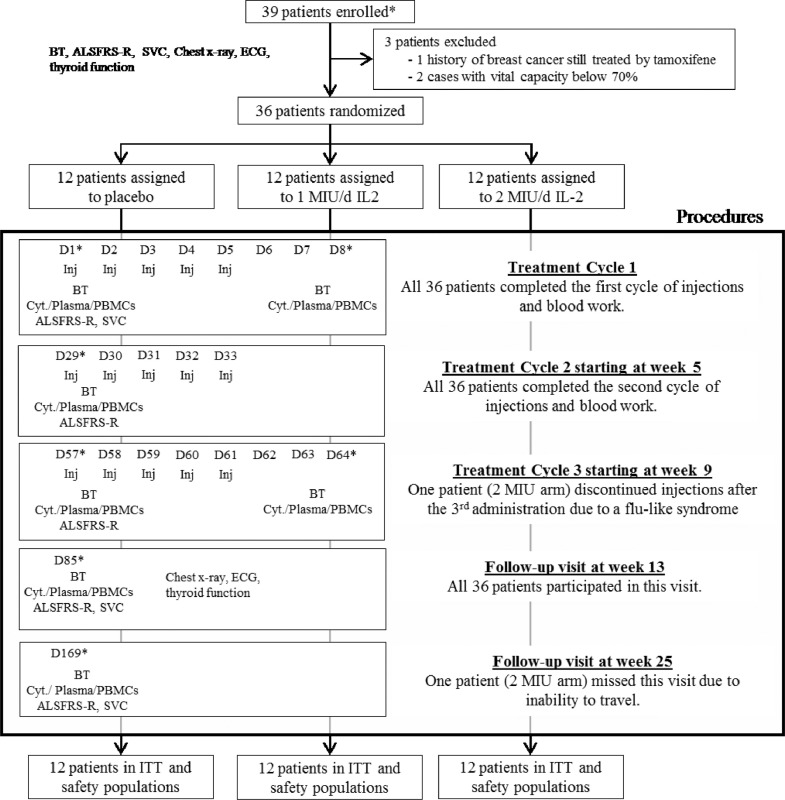
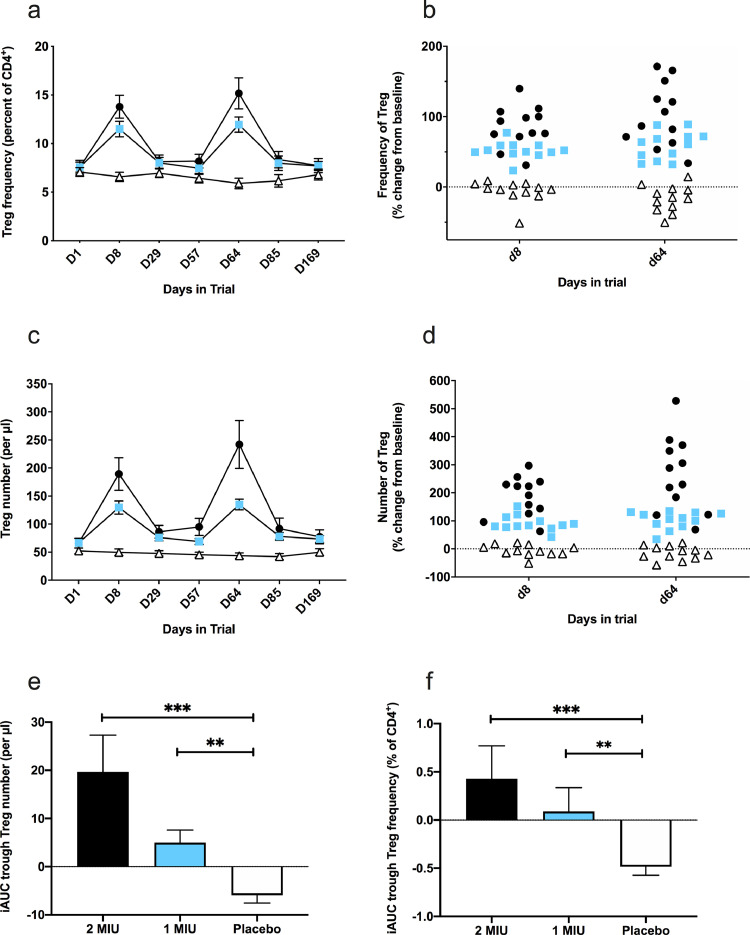
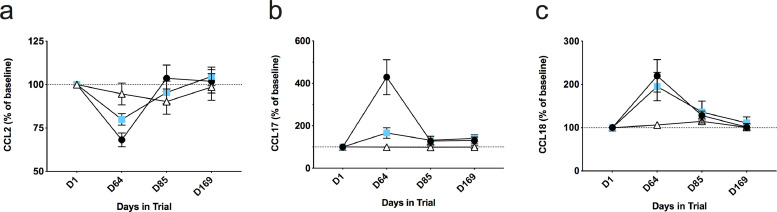
Methods: We performed a single centre, parallel three-arm, randomised, double-blind, placebo-controlled study. Eligibility criteria included age < 75 years, disease duration < 5 years, riluzole treatment > 3 months, and a slow vital capacity ≥ 70% of normal. Patients were randomised (1:1:1) to aldesleukin 2 MIU, 1 MIU, or placebo once daily for 5 days every 4 weeks for 3 cycles. Primary outcome was change from baseline in Treg percentage of CD4+ T cells (%Tregs) following a first cycle. Secondary laboratory outcomes included: %Treg and Treg number following repeated cycles, and plasma CCL2 and neurofilament light chain protein (NFL) concentrations as surrogate markers of efficacy. Safety outcomes included motor-function (ALSFRS-R), slow vital capacity (SVC), and adverse event reports. This trial is registered with ClinicalTrials.gov, NCT02059759.
Findings: All randomised patients (12 per group), recruited from October 2015 to December 2015, were alive at the end of follow-up and included in the intent-to-treat (ITT) analysis. No drug-related serious adverse event was observed. Non-serious adverse events occurred more frequently with the 1 and 2 MIU IL-2 doses compared to placebo, including injection site reactions and flu-like symptoms. Primary outcome analysis showed a significant increase (p < 0·0001) in %Tregs in the 2 MIU and 1 MIU arms (mean [SD]: 2 MIU: +6·2% [2·2]; 1 MIU: +3·9% [1·2]) as compared to placebo (mean [SD]: -0·49% [1·3]). Effect sizes (ES) were large in treated groups: 2 MIU ES=3·7 (IC95%: 2·3-4·9) and 1 MIU ES=3·5 (IC95%: 2·1-4·6). Secondary outcomes showed a significant increase in %Tregs following repeated cycles (p < 0·0001) as compared to placebo, and a dose-dependent decrease in plasma CCL2 (p = 0·0049). There were no significant differences amongst the three groups on plasma NFL levels.
Interpretation: Ld-IL-2 is well tolerated and immunologically effective in subjects with ALS. These results warrant further investigation into their eventual therapeutic impact on slowing ALS disease progression.
Funding: The French Health Ministry (PHRC-I-14-056), EU H2020 (grant #633413), and the Association pour la Recherche sur la SLA (ARSLA).
Keywords: Amyotrophic lateral sclerosis; Biomarkers; Low dose interleukin-2; Neuro-inflammation; Randomised clinical trial; Regulatory T cells.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest Drs. Camu, Mickunas, Payan, Juntas Morales, Pageot, Masseguin, Suehs, De Vos, Saker, Andreasson and Veyrune have nothing to disclose. Dr. Bensimon reports grants from French Health Ministry (PHRC-I), ARSLA and EU HORIZON 2020, during the conduct of the study; in addition, Dr. Bensimon has a patent (WO 2012123381 A1) with royalties paid to Assistance Publique Hopitaux de Paris (APHP), Institut National de la Sante et de la Recherche Medicale INSERM, and Sorbonne Universite. Drs. Bensimon, Tree, Leigh, Locati, Garlanda, Shaw, Kirby, Malaspina have a patent (B75649EPD40021) pending. Dr. Malaspina reports grants from EU HORIZON 2020, grants from MND Association UK, grants and other from Barts and the London Charity, and from UCB Pharma SPRL, during the conduct of the study; and from F. Hoffmann-La Roche outside the submitted work. Dr. Zetterberg reports personal fees from Samumed, Roche Diagnostics, Denali, CogRx and Wave, outside the submitted work. Dr. Kirby reports grants from The Nimes University Hospital Center (CHU Nimes) and grants from EU HORIZON 2020, during the conduct of the study. Dr. Shaw reports grants from EU HORIZON 2020, Sheffield component and MIROCALS (633413), outside the submitted work. Dr. Al-Chalabi reports involvement as Chief Investigator for LEVALS clinical trial and European CI for REFALS clinical trial for OrionPharma, as well as consultancy from Mitsubishi Tanabe Pharma, consultancy and involvement in debating panel for Cytokinetics Inc, consultancy from Chronos Therapeutics, GSK, Lilly, and from Biogen Idec, outside the submitted work.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
