

Proof-of-principle Phase I results of combining nivolumab with brachytherapy and external beam radiation therapy for Grade Group 5 prostate cancer: safety, feasibility, and exploratory analysis
- PMID: 32651467
- PMCID: PMC7882397
- DOI: 10.1038/s41391-020-0254-y
Proof-of-principle Phase I results of combining nivolumab with brachytherapy and external beam radiation therapy for Grade Group 5 prostate cancer: safety, feasibility, and exploratory analysis
Abstract
Background: To determine whether combining brachytherapy with immunotherapy is safe in prostate cancer (PCa) and provides synergistic effects, we performed a Phase I/II trial on the feasibility, safety, and benefit of concurrent delivery of anti-PD-1 (nivolumab) with high-dose-rate (HDR) brachytherapy and androgen deprivation therapy (ADT) in patients with Grade Group 5 (GG5) PCa.
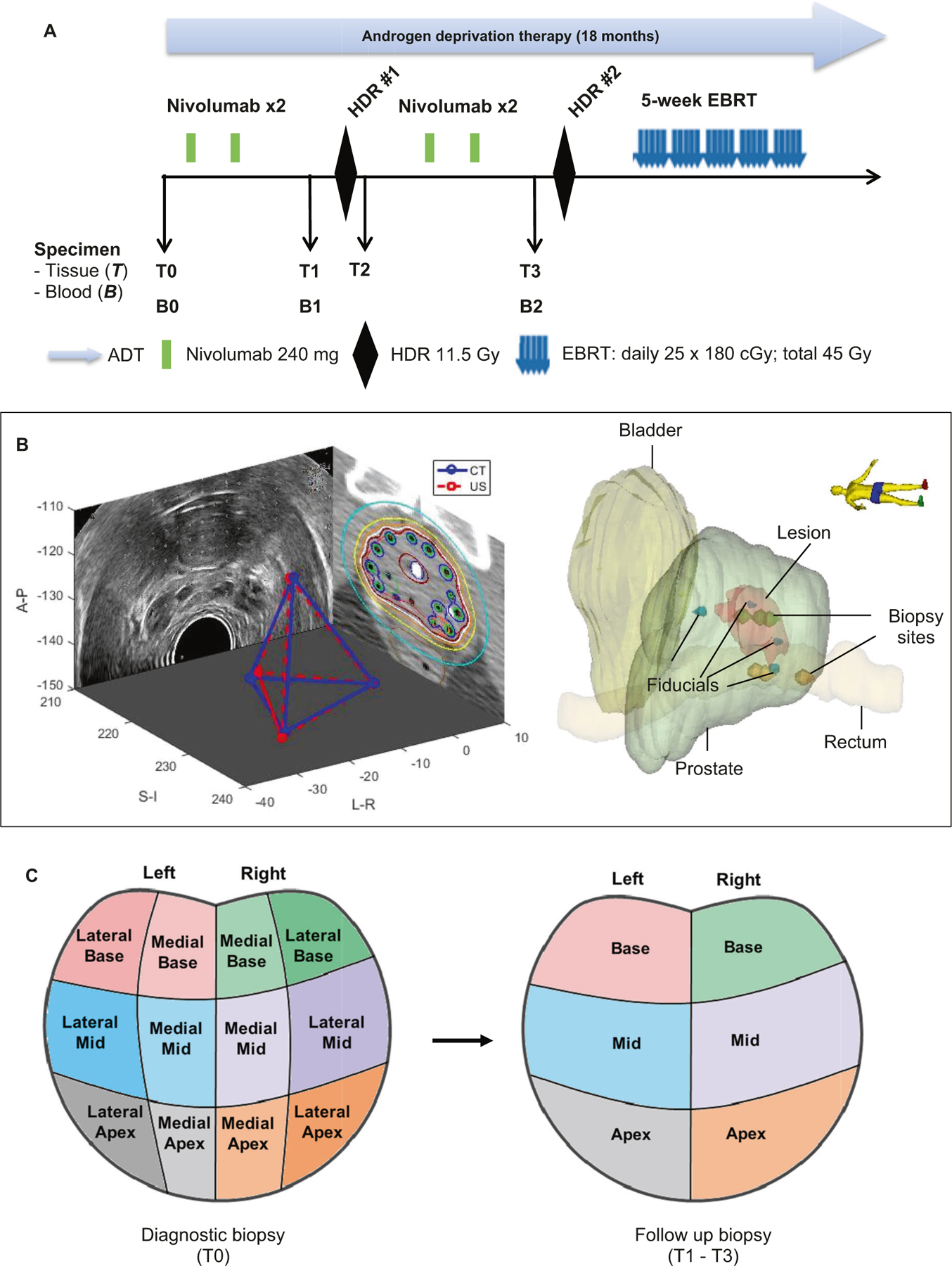
Methods: Eligible patients were aged 18 years or older with diagnosis of GG5 PCa. Patients received ADT, nivolumab every two weeks for four cycles, with two cycles prior to first HDR, and two more cycles prior to second HDR, followed by external beam radiotherapy. The primary endpoint was to determine safety and feasibility. This Phase I/II trial is registered with ClinicalTrials.gov (NCT03543189).
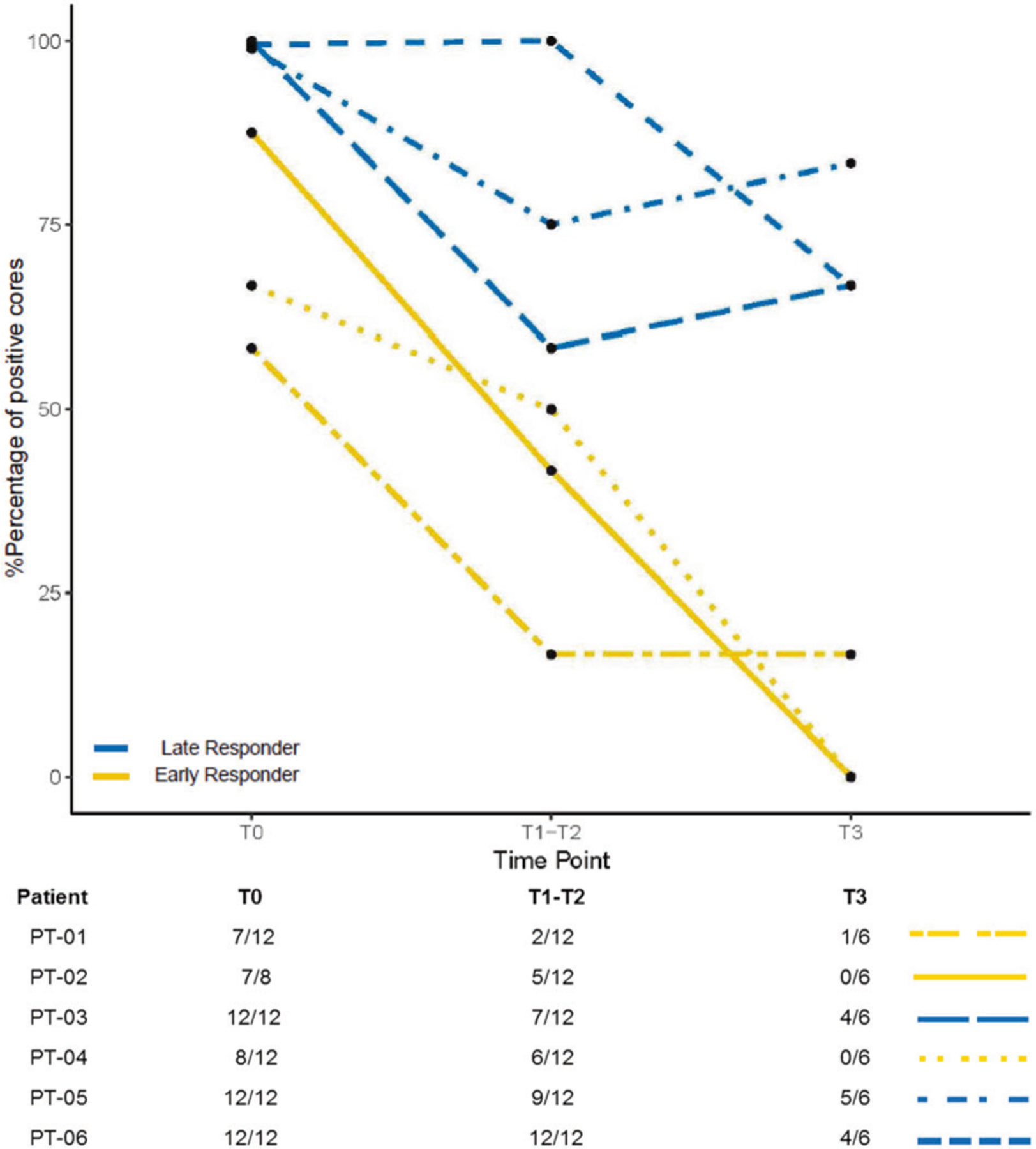
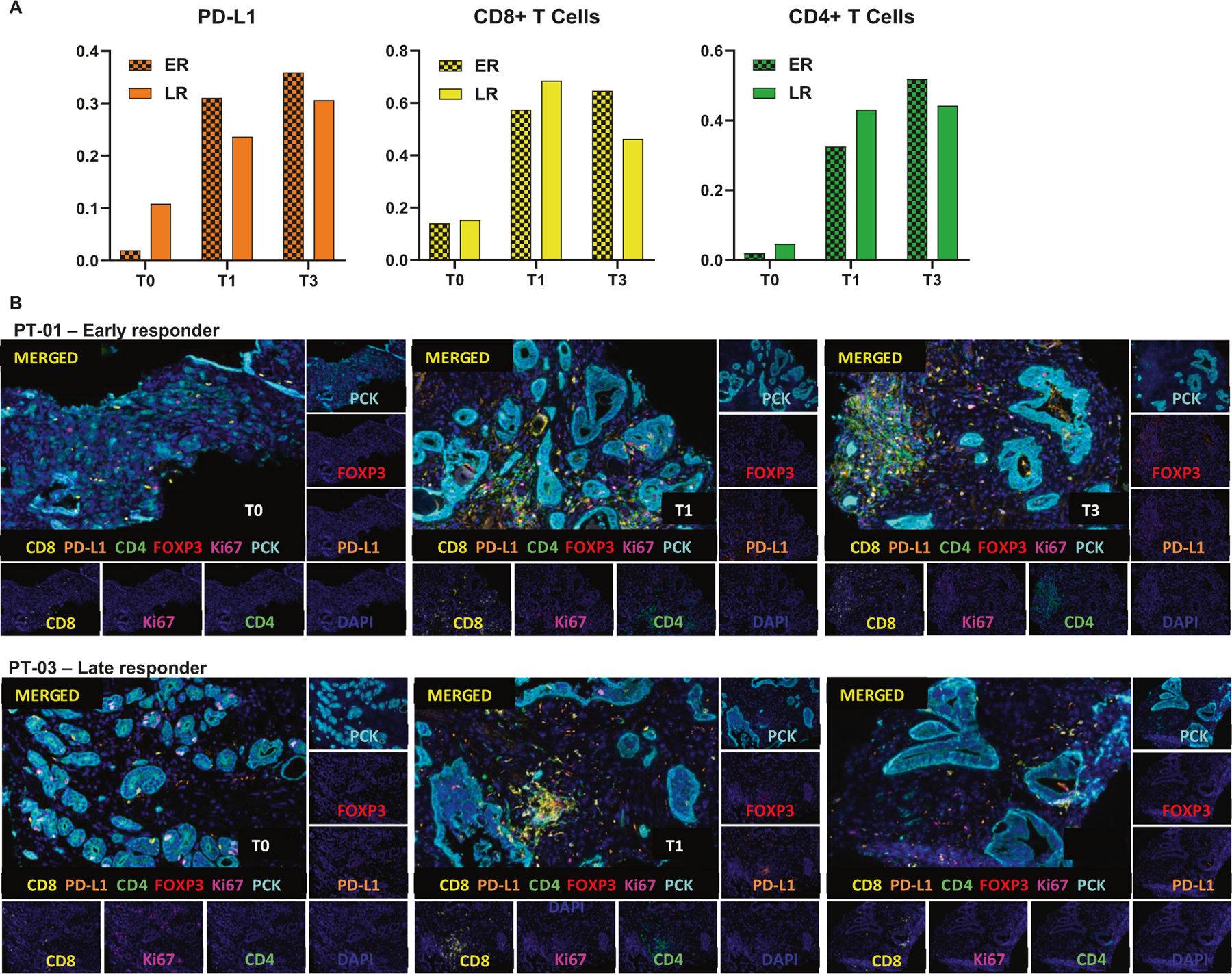
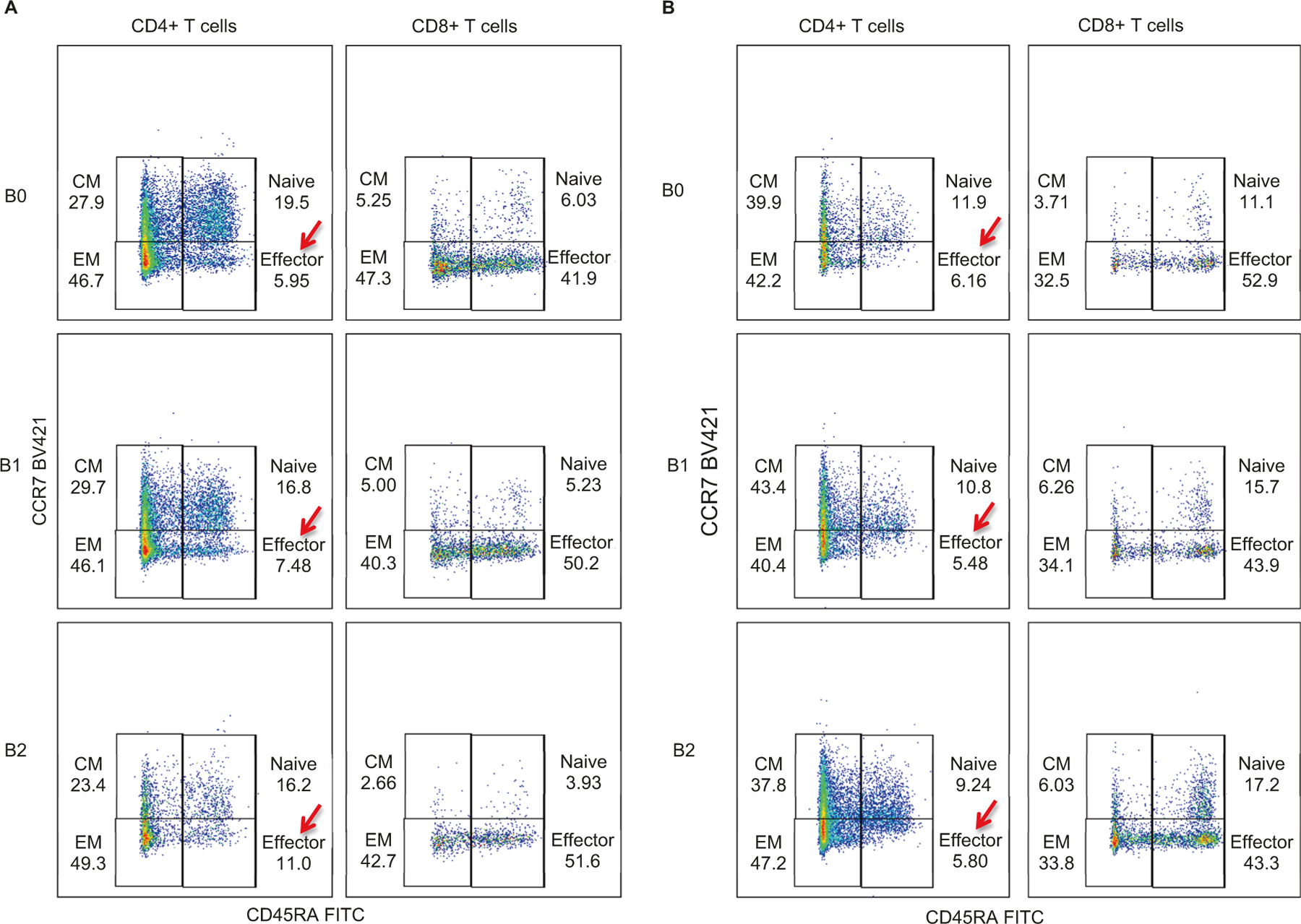
Results: Between September 2018 and June 2019, six patients were enrolled for the Phase I safety lead-in with a minimum observation period of 3 months after nivolumab administration. Overall, nivolumab was well tolerated in combination with ADT and HDR treatment. One patient experienced a grade 3 dose-limiting toxicity (elevated Alanine aminotransferase and Aspartate aminotransferase) after the second cycle of nivolumab. Three patients (50%) demonstrated early response with no residual tumor detected in ≥4 of 6 cores on biopsy post-nivolumab (4 cycles) and 1-month post-HDR. Increase in CD8+ and FOXP3+/CD4+ T cells in tissues, and CD4+ effector T cells in peripheral blood were observed in early responders.
Conclusion: Combination of nivolumab with ADT and HDR is well tolerated and associated with evidence of increased immune infiltration and antitumor activity.
Conflict of interest statement
Figures
References
-
- Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl J Med 2015;372:2018–28. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
