

Review
doi: 10.1038/s41575-020-0347-z.
COVID-19 and liver transplantation
Affiliations
- PMID: 32651555
- PMCID: PMC7351540
- DOI: 10.1038/s41575-020-0347-z
Item in Clipboard
Review
COVID-19 and liver transplantation
Nat Rev Gastroenterol Hepatol.
2020 Sep.
Abstract
The effect of coronavirus disease 2019 (COVID-19) on liver transplantation programmes and recipients is still not completely understood but overall involves the risk of donor-derived transmission, the reliability of diagnostic tests, health-care resource utilization and the effect of immunosuppression. This Comment reviews the effect of COVID-19 on liver transplantation and summarizes recommendations for donor and recipient management.
Conflict of interest statement
The authors declare no competing interests.
Figures
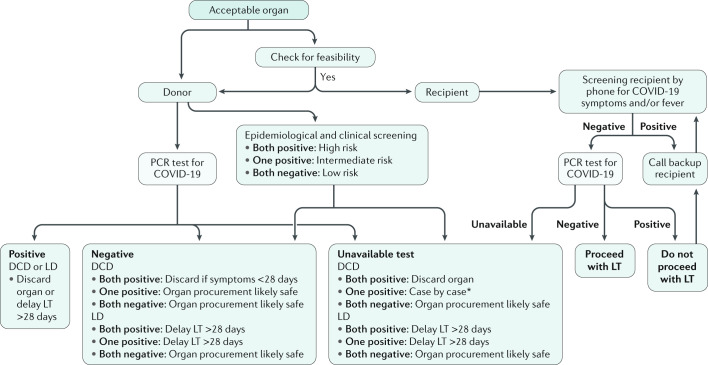
Epidemiological screening includes any of the following: travel or residence in a high-risk area, contact with a suspected case of coronavirus disease 2019 (COVID-19) ≤21 days before, or contact with a confirmed case of COVID-19 ≤28 days before. Clinical screening includes onset of any of the following symptoms 21 days before evaluation: fever >38 °C; malaise or flu-like symptoms; new cough; shortness of breath; unexplained abdominal pain, nausea or diarrhoea; or loss of sense of taste or smell. *Liver transplantation (LT) decision should be made with caution and at least 28 days after presumptive diagnosis of COVID-19. Figure is based on the main international transplant societies’ recommendations (such as AST and AASLD). DCD, deceased donor; LD, living donor. For further details, see Supplementary Box 1.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
