

The Effect of Tumor Size and Histologic Findings on Outcomes After Segmentectomy vs Lobectomy for Clinically Node-Negative Non-Small Cell Lung Cancer
- PMID: 32652096
- PMCID: PMC7856530
- DOI: 10.1016/j.chest.2020.06.066
The Effect of Tumor Size and Histologic Findings on Outcomes After Segmentectomy vs Lobectomy for Clinically Node-Negative Non-Small Cell Lung Cancer
Abstract
Background: The interaction between tumor size and the comparative prognosis of lobar and sublobar resection has been defined poorly.
Research question: The purpose of this study was to characterize the relationship between tumor size and the receipt of segmentectomy or lobectomy in association with overall survival in patients with clinically node-negative non-small cell lung cancer (NSCLC).
Study design and methods: The 2004-2015 National Cancer Database (NCDB) was queried for patients with cT1-3N0M0 NSCLC who underwent segmentectomy or lobectomy without neoadjuvant therapy or missing survival data. The primary outcome was overall survival, which was evaluated using multivariate Cox proportional hazards including an interaction term between tumor size and type of surgery.
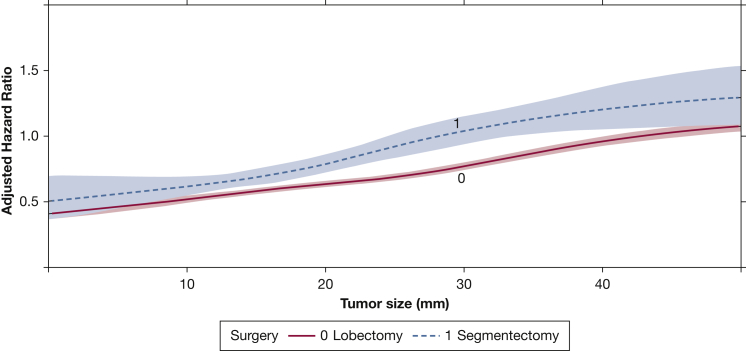
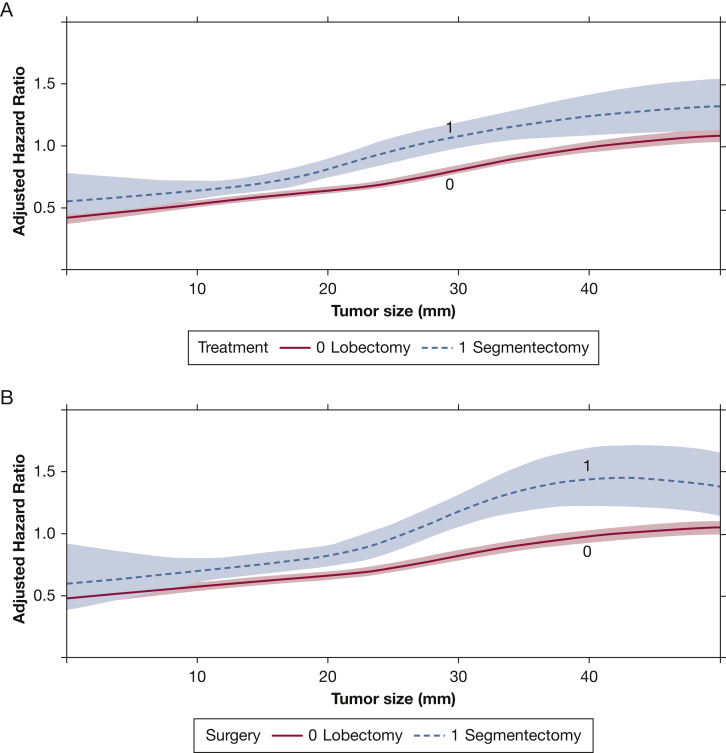
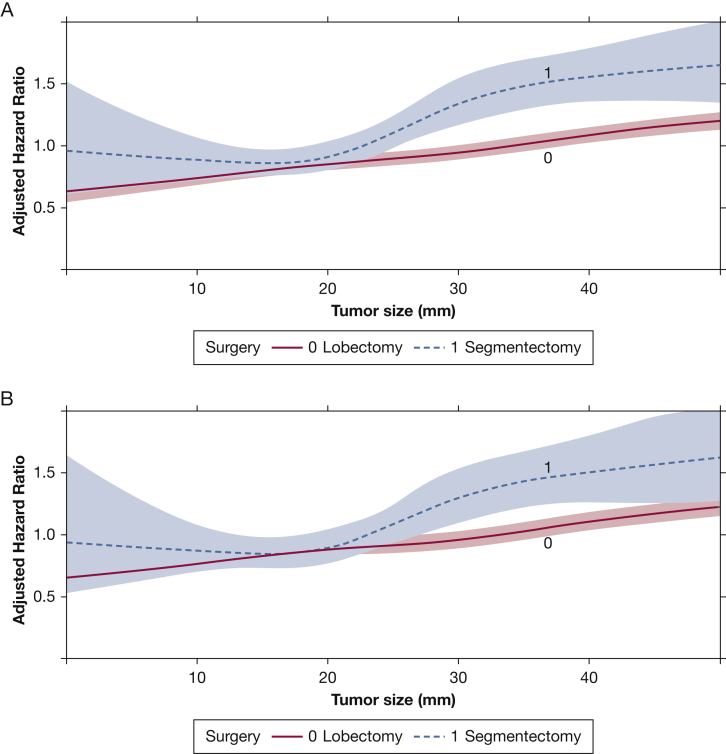
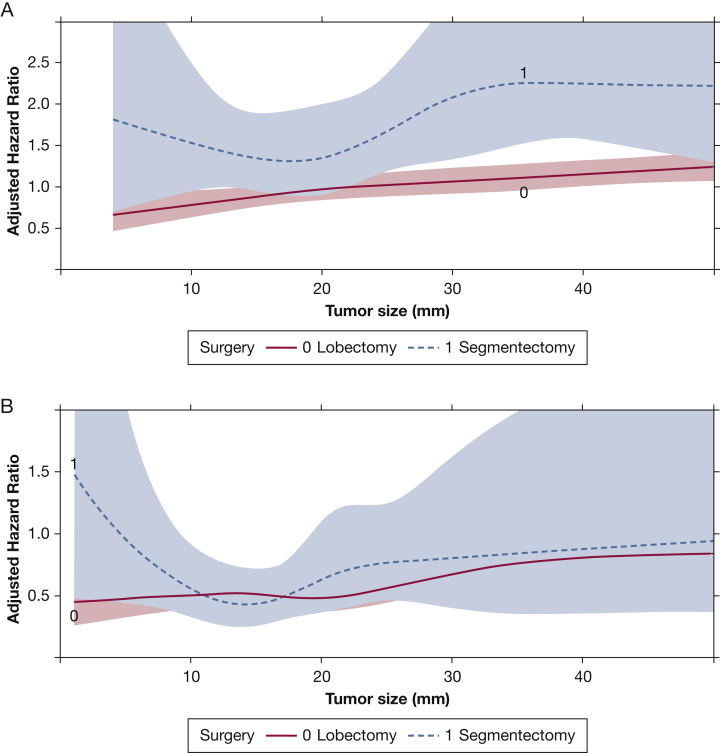
Results: A total of 143,040 patients were included: 135,446 (95%) underwent lobectomy and 7594 (5%) underwent segmentectomy. In multivariate Cox regression, a significant three-way interaction was found among tumor size, histologic results, and type of surgery (P < .001). When patients were stratified by histologic results, lobectomy was associated with significantly improved survival compared with segmentectomy beyond a tumor size of approximately 10 mm for adenocarcinoma and 15 mm for squamous cell carcinoma that was recapitulated in subgroup analyses. No interaction between tumor size and type of surgery was found for patients with neuroendocrine tumors.
Interpretation: In this NCDB study of patients with node-negative NSCLC, we found different tumor size thresholds, based on histologic results, that identified populations of patients who least and most benefitted from lobectomy compared with segmentectomy.
Keywords: lobectomy; non-small cell lung cancer; sublobar resection; surgery.
Copyright © 2020 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Comparing Outcomes of Segmentectomy and Lobectomy for Non-small Cell Lung Cancer: Is Less Truly More?Chest. 2021 Jan;159(1):21-22. doi: 10.1016/j.chest.2020.07.063. Chest. 2021. PMID: 33422198 No abstract available.
-
How to Select Patients With Clinically Early-Stage Non-Small Cell Lung Cancer for Segmentectomy?Chest. 2021 Jan;159(1):444-445. doi: 10.1016/j.chest.2020.07.083. Chest. 2021. PMID: 33422216 No abstract available.
-
Response.Chest. 2021 Jan;159(1):445-446. doi: 10.1016/j.chest.2020.08.2044. Chest. 2021. PMID: 33422217 No abstract available.
References
-
- Dai C., Shen J., Ren Y. Choice of surgical procedure for patients with non-small-cell lung cancer ≤ 1 cm or > 1 to 2 cm among lobectomy, segmentectomy, and wedge resection: a population-based study. J Clin Oncol. 2016;34(26):3175–3182. - PubMed
-
- Kamel M.K., Rahouma M., Lee B. Segmentectomy is equivalent to lobectomy in hypermetabolic clinical stage IA lung adenocarcinomas. Ann Thorac Surg. 2019;107(1):217–223. - PubMed
-
- Zhao Z.-R., Situ D.-R., Lau R.W.H. Comparison of segmentectomy and lobectomy in stage IA adenocarcinomas. J Thorac Oncol. 2017;12(5):890–896. - PubMed
-
- Dziedzic R., Zurek W., Marjanski T. Stage I non-small-cell lung cancer: long-term results of lobectomy versus sublobar resection from the Polish National Lung Cancer Registry. Eur J Cardiothorac Surg. 2017;52(2):363–369. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
