

Intestinal Virome Signature Associated With Severity of Nonalcoholic Fatty Liver Disease
- PMID: 32652145
- PMCID: PMC8404510
- DOI: 10.1053/j.gastro.2020.07.005
Intestinal Virome Signature Associated With Severity of Nonalcoholic Fatty Liver Disease
Abstract
Background & aims: Alterations in the gut microbiome have been associated with the severity of nonalcoholic fatty liver disease (NAFLD). Previous studies focused exclusively on the bacteria in the microbiome; we investigated changes in the viral microbiome (virome) in patients with NAFLD.
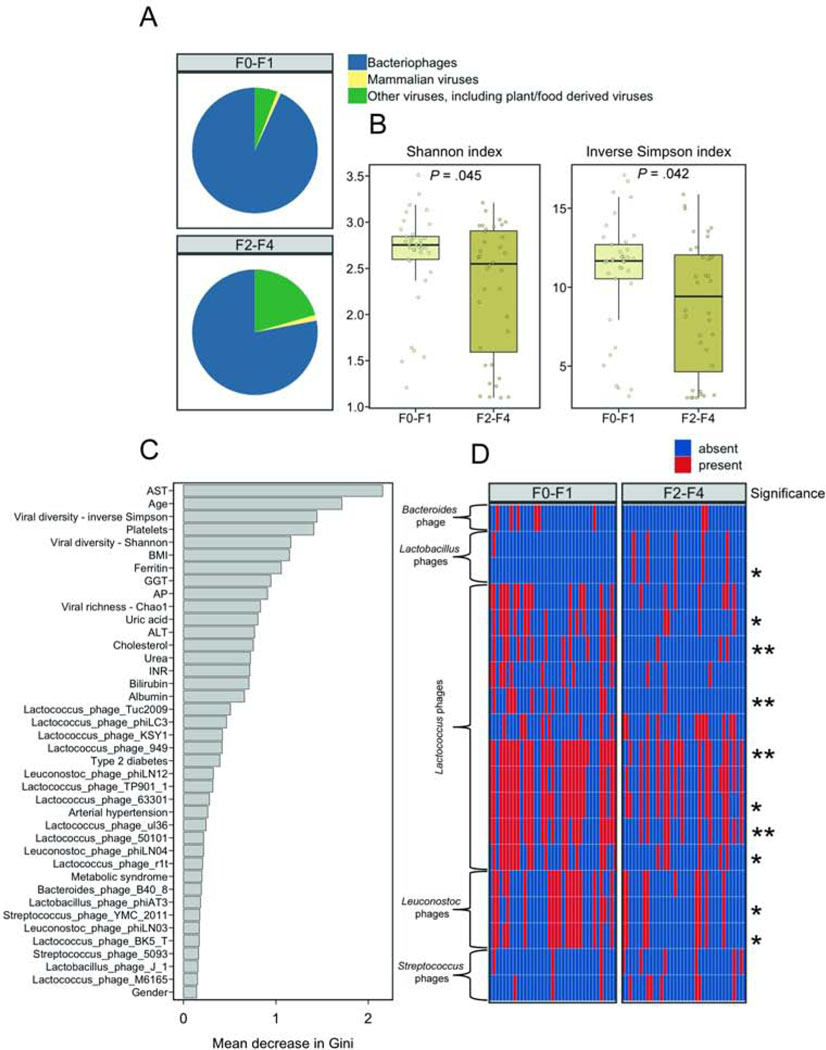
Methods: In a prospective, cross-sectional, observational study, we extracted RNA and DNA virus-like particles from fecal samples from 73 patients with NAFLD: 29 patients had an NAFLD Activity Score (NAS) of 0-4, 44 patients had an NAS of 5-8 or liver cirrhosis (LCI), 37 patients had F0-F1 fibrosis, and 36 patients had F2-F4 fibrosis. As controls, 9 individuals without liver disease and 13 patients with mild primary biliary cholangitis were included in the analysis. We performed shotgun metagenomic sequencing of virus-like particles.
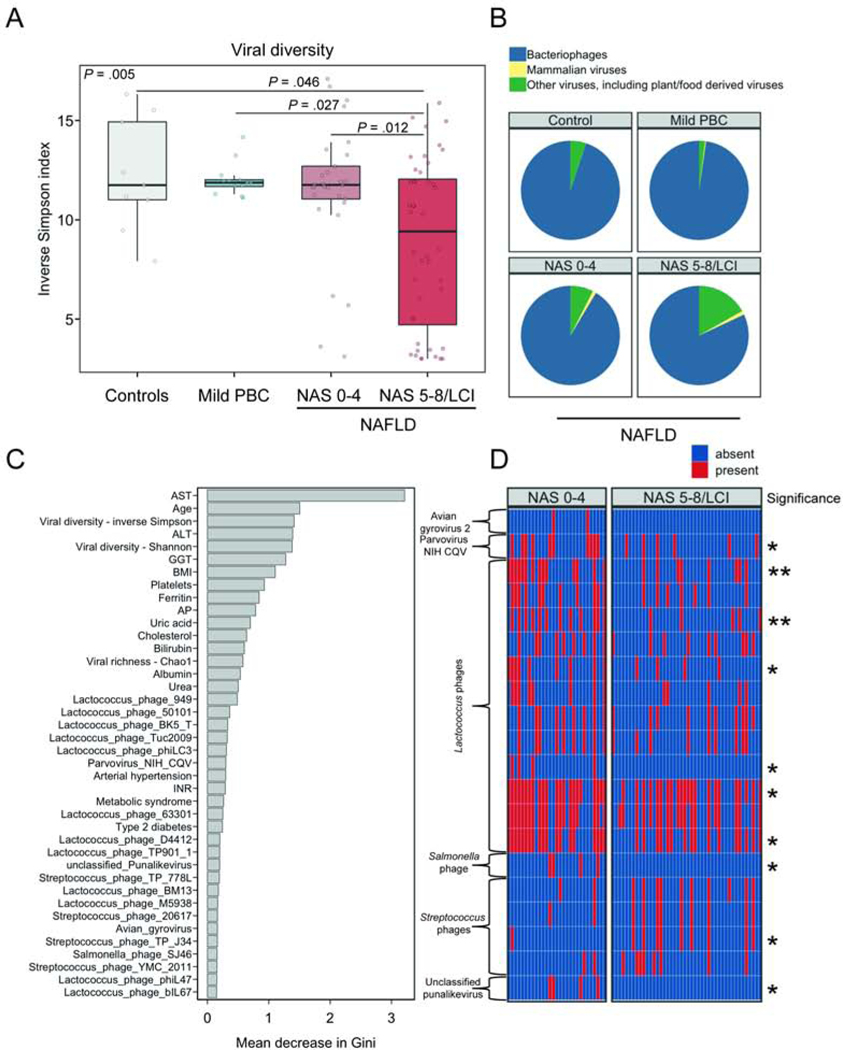
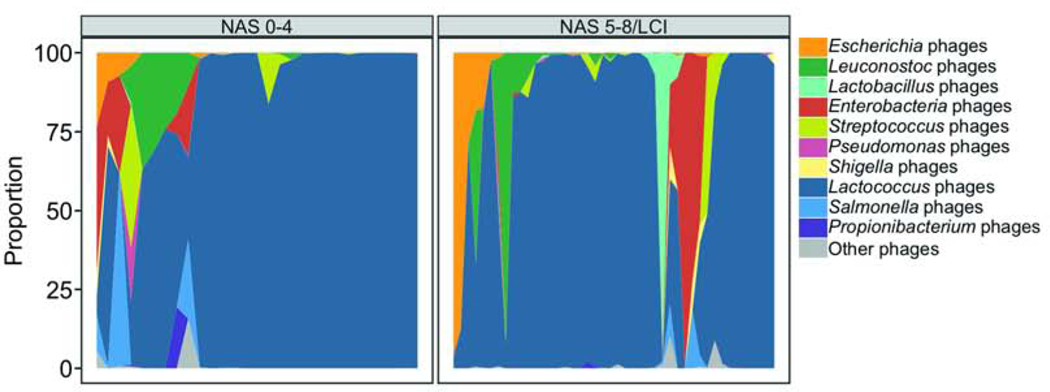
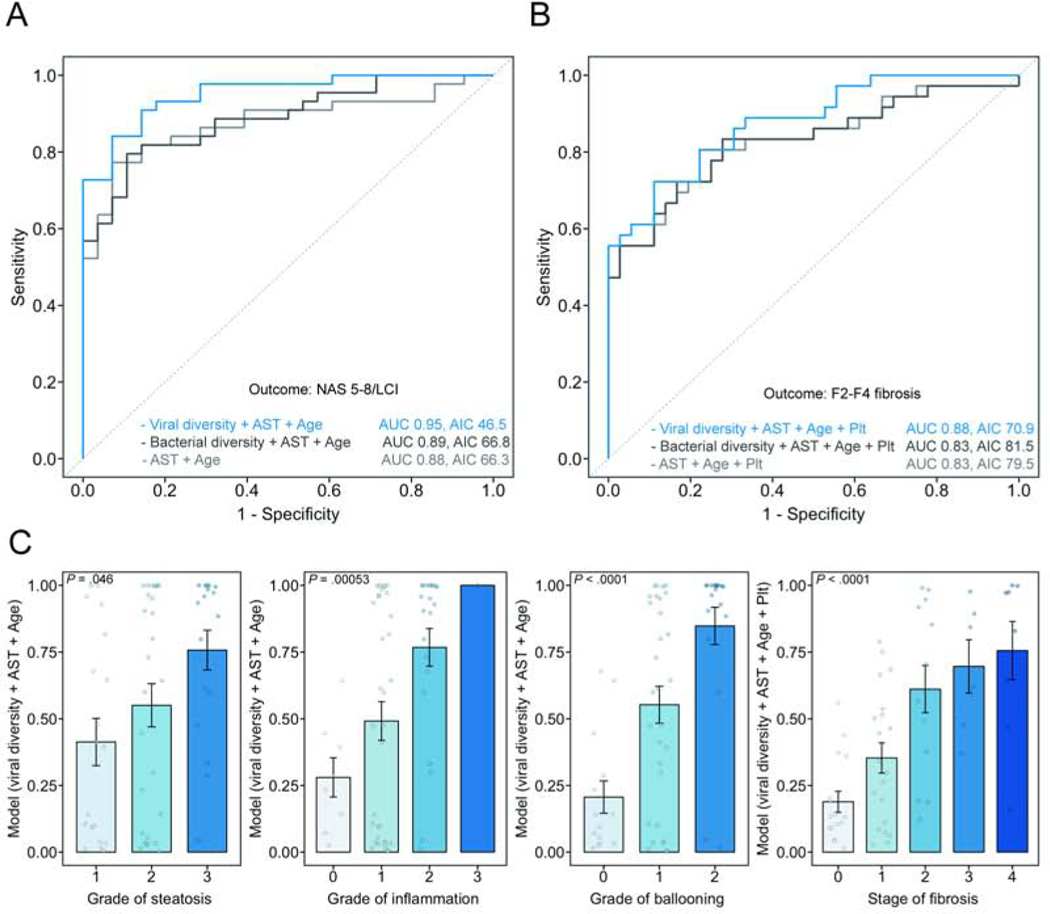
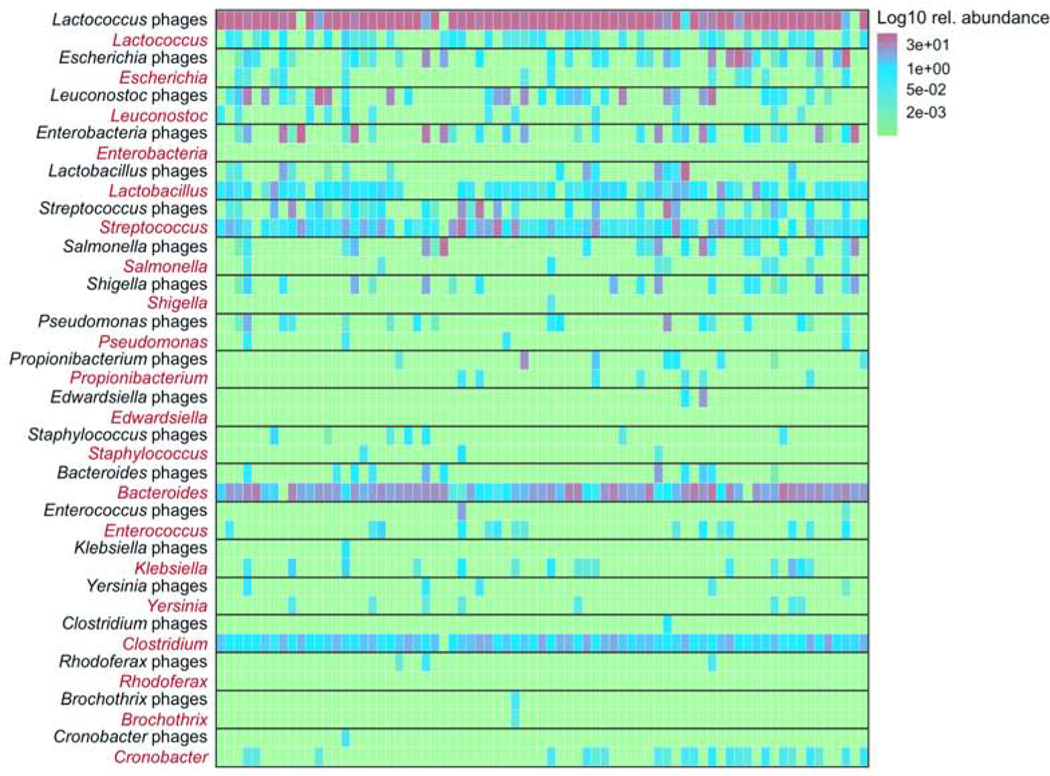
Results: Patients with NAFLD and NAS 5-8/LCI had a significant decrease in intestinal viral diversity compared with patients with NAFLD and NAS 0-4 or control individuals. The presence of more advanced NAFLD was associated with a significant reduction in the proportion of bacteriophages compared with other intestinal viruses. Using multivariate logistic regression analysis with leave-1-out cross validation, we developed a model, including a viral diversity index and simple clinical variables, that identified patients with NAS 5-8/LCI with an area under the curve of 0.95 (95% confidence interval, 0.91-0.99) and F2-F4 fibrosis with an area under the curve of 0.88 (95% confidence interval, 0.80-0.95). Addition of data on viral diversity significantly improved multivariate models, including those based on only clinical parameters or bacterial diversity.
Conclusions: In a study of fecal viromes from patients with NAFLD and control individuals, we associated histologic markers of NAFLD severity with significant decreases in viral diversity and proportion of bacteriophages. We developed a model based on fecal viral diversity and clinical data that identifies patients with severe NAFLD and fibrosis more accurately than models based only on clinical or bacterial data.
Keywords: Biomarker; Microbiota; Prognostic Factor; Progression.
Published by Elsevier Inc.
Figures
References
-
- Diehl AM, Day C. Cause, Pathogenesis, and Treatment of Nonalcoholic Steatohepatitis. N Engl J Med 2017;377:2063–2072. - PubMed
-
- Ekstedt M, Hagström H, Nasr P, et al.Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015;61:1547–1554. - PubMed
-
- Vilar-Gomez E, Chalasani N. Non-invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J Hepatol 2018;68:305–315. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
