

Tumour budding, poorly differentiated clusters, and T-cell response in colorectal cancer
- PMID: 32652320
- PMCID: PMC7347996
- DOI: 10.1016/j.ebiom.2020.102860
Tumour budding, poorly differentiated clusters, and T-cell response in colorectal cancer
Abstract
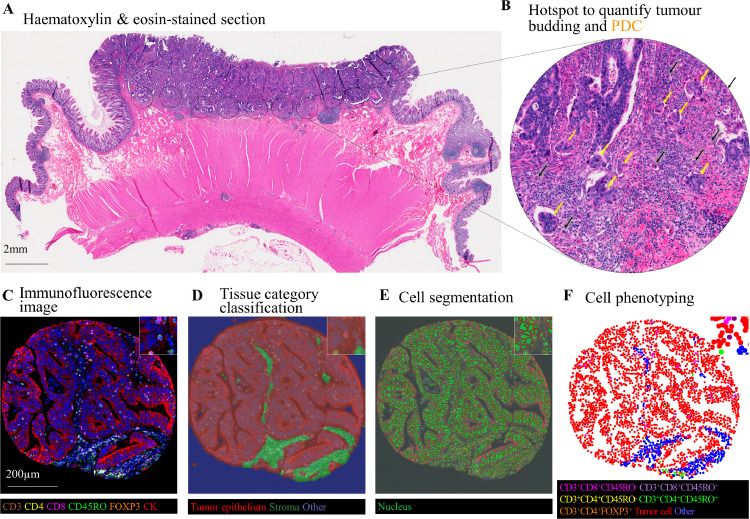
Background: Tumour budding and poorly differentiated clusters (PDC) represent forms of tumour invasion. We hypothesised that T-cell densities (reflecting adaptive anti-tumour immunity) might be inversely associated with tumour budding and PDC in colorectal carcinoma.
Methods: Utilising 915 colon and rectal carcinomas in two U.S.-wide prospective cohort studies, and multiplex immunofluorescence combined with machine learning algorithms, we assessed CD3, CD4, CD8, CD45RO (PTPRC), and FOXP3 co-expression patterns in lymphocytes. Tumour budding and PDC at invasive fronts were quantified by digital pathology and image analysis using the International tumour Budding Consensus Conference criteria. Using covariate data of 4,420 incident colorectal cancer cases, inverse probability weighting (IPW) was integrated with multivariable logistic regression analysis that assessed the association of T-cell subset densities with tumour budding and PDC while adjusting for selection bias due to tissue availability and potential confounders, including microsatellite instability status.
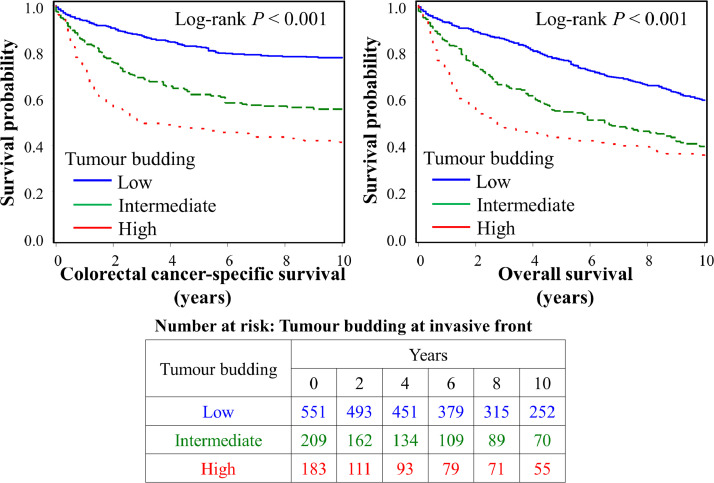
Findings: Tumour budding counts were inversely associated with density of CD3+CD8+ [lowest vs. highest: multivariable odds ratio (OR), 0.50; 95% confidence interval (CI), 0.35-0.70; Ptrend < 0.001] and CD3+CD8+CD45RO+ cells (lowest vs. highest: multivariable OR, 0.44; 95% CI, 0.31-0.63; Ptrend < 0.001) in tumour epithelial region. Tumour budding levels were associated with higher colorectal cancer-specific mortality (multivariable hazard ratio, 2.13; 95% CI, 1.57-2.89; Ptrend < 0.001) in Cox regression analysis. There were no significant associations of PDC with T-cell subsets.
Interpretation: Tumour epithelial naïve and memory cytotoxic T cell densities are inversely associated with tumour budding at invasive fronts, suggesting that cytotoxic anti-tumour immunity suppresses tumour microinvasion.
Keywords: adenocarcinoma; artificial intelligence; clinical outcomes; epithelial mesenchymal transition; host-tumour interaction; molecular pathological epidemiology.
Copyright © 2020. Published by Elsevier B.V.
Figures
Comment in
-
The battle for prognosis at the invasive front of colorectal cancer.EBioMedicine. 2020 Aug;58:102918. doi: 10.1016/j.ebiom.2020.102918. Epub 2020 Jul 22. EBioMedicine. 2020. PMID: 32711249 Free PMC article. No abstract available.
References
-
- Zlobec I., Lugli A. Tumour budding in colorectal cancer: molecular rationale for clinical translation. Nat Rev Cancer. 2018;18(4):203–204. - PubMed
-
- Lugli A., Kirsch R., Ajioka Y., Bosman F., Cathomas G., Dawson H. Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod Pathol. 2017;30(9):1299–1311. - PubMed
-
- Ueno H., Kajiwara Y., Shimazaki H., Shinto E., Hashiguchi Y., Nakanishi K. New criteria for histologic grading of colorectal cancer. Am J Surg Pathol. 2012;36(2):193–201. - PubMed
MeSH terms
Substances
Grants and funding
- R35 CA197735/CA/NCI NIH HHS/United States
- R01 CA118553/CA/NCI NIH HHS/United States
- P01 CA087969/CA/NCI NIH HHS/United States
- R01 CA248857/CA/NCI NIH HHS/United States
- R37 CA225655/CA/NCI NIH HHS/United States
- U01 CA167552/CA/NCI NIH HHS/United States
- R01 CA137178/CA/NCI NIH HHS/United States
- K24 DK098311/DK/NIDDK NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- R01 CA169141/CA/NCI NIH HHS/United States
- P50 CA127003/CA/NCI NIH HHS/United States
- P01 CA055075/CA/NCI NIH HHS/United States
- R01 CA151993/CA/NCI NIH HHS/United States
- K07 CA188126/CA/NCI NIH HHS/United States
- UM1 CA167552/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
