

Management and outcomes of heart failure patients with CKD: experience from an inter-disciplinary clinic
- PMID: 32652822
- PMCID: PMC7524254
- DOI: 10.1002/ehf2.12796
Management and outcomes of heart failure patients with CKD: experience from an inter-disciplinary clinic
Abstract
Aims: CKD-HF patients suffer excess hospitalization and mortality, often under-treated with life-prolonging medications due to fear of worsening renal function and hyperkalaemia. Yet, role of inter-disciplinary working in improving therapy is unknown, which this study aims to investigate.
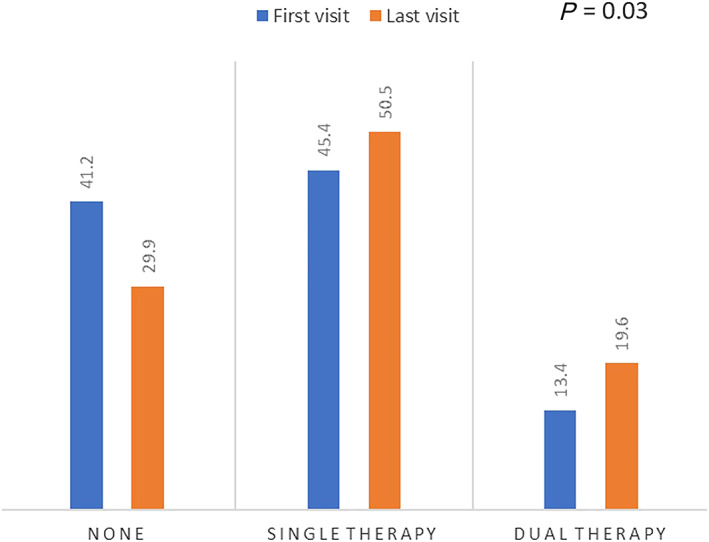
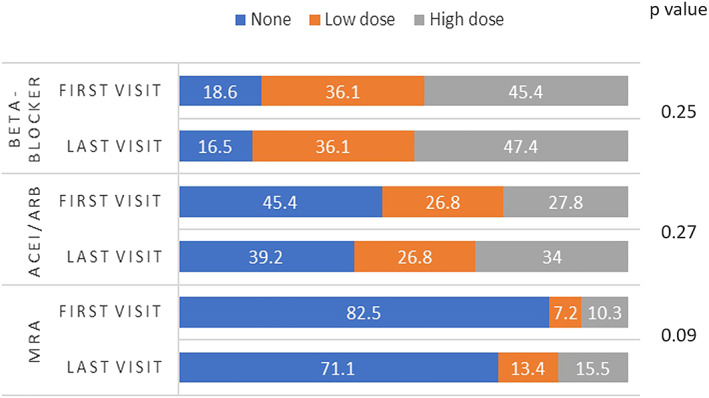
Methods and results: Clinical, biochemical data, and medications at first and last clinic visit were obtained from patient records for 124 patients seen in kidney failure-heart failure clinic (23 March 2017 to 11 April 2019). Medication dose groups (none, low, and high dose), number of RAASi agents, and blood test results were compared between first and last visit in patients with at least two clinic visits (n = 97). Patient characteristics were age 78.5 years (IQR 68.1-84.4 years), male 67.7%, diabetes 51.6%, moderate (45.2%) vs. severe (39.5%) CKD, HF with reduced ejection fraction (HFrEF) (49.2%), follow-up 234 days (IQR 121-441 days). HFrEF was associated with increased risk of death (adjusted OR 4.49, 95% CI 1.43-14.05; P = 0.01). Distributions of patients according to number of RAASi agents they were on differed between first and last visit (P = 0.03). Dosage was increased in 25.9% for beta-blockers, 33.0% for ACEi/ARBs, and 17.5% for MRAs. Distributions of patients across MRA dosage groups was different (P = 0.03), with higher proportions on higher dosages at last visit, without significant changes in serum potassium or creatinine. Serum ferritin improved (131.0 vs. 267.5 μg/L; P < 0.001), and fewer patients had iron deficiency (56.7% vs. 26.8%; P = 0.002) at last visit compared to the first.
Conclusions: This inter-disciplinary clinic improved guideline-recommended medication prescription, MRA dosages in CKD-HF patients without significant biochemical abnormality, and iron status. A prospectively designed study with medication titration protocol and defined patient-centred outcomes is needed to further assess effectiveness of such clinic.
Keywords: Aldosterone antagonists; Angiotensin converting enzyme inhibitors; Chronic kidney disease; Heart failure; Kidney failure; Systolic heart failure.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
DB has received Grants from British Heart Foundation PG 10/71/28462 and partially funded for this work by Welcome ISSF; DB has received Honoraria from Pfizer, ViforPharma and AstraZeneca.
MN was partially funded by George's Academic Training (GAT).
Figures
References
-
- Damman K, Tang WHW, Felker GM, Lassus J, Zannad F, Krum H, McMurray JJV. Current evidence on treatment of patients with chronic systolic heart failure and renal insufficiency: practical considerations from published data. J Am Coll Cardiol 2014; 63: 853–871. - PubMed
-
- Heywood JT, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, McBride ML, Mehra MR, O'Connor CM, Reynolds D, Walsh MN. Influence of renal function on the use of guideline‐recommended therapies for patients with heart failure. Am J Cardiol 2010; 105: 1140–1146. - PubMed
-
- House AA, Wanner C, Sarnak MJ, Piña IL, McIntyre CW, Komenda P, Kasiske BL, Deswal A, deFilippi CR, Cleland JGF, Anker SD, Herzog CA, Cheung M, Wheeler DC, Winkelmayer WC, McCullough PA, Abu‐Alfa AK, Amann K, Aonuma K, Appel LJ, Baigent C, Bakris GL, Banerjee D, Boletis JN, Bozkurt B, Butler J, Chan CT, Costanzo MR, Dubin RF, Filippatos G, Gikonyo BM, Gikonyo DK, Hajjar RJ, Iseki K, Ishii H, Knoll GA, Lenihan CR, Lentine KL, Lerma EV, Macedo E, Mark PB, Noiri E, Palazzuoli A, Pecoits‐Filho R, Pitt B, Rigatto C, Rossignol P, Setoguchi S, Sood MM, Störk S, Suri RS, Szummer K, Tang SCW, Tangri N, Thompson A, Vijayaraghavan K, Walsh M, Wang AYM, Weir MR. Heart failure in chronic kidney disease: conclusions from a kidney disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2019; 95: 1304–1317. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2016; 37: 2129–2200.
-
- Hemmelgarn BR, Manns BJ, Zhang J, Tonelli M, Klarenbach S, Walsh M, Culleton BF. Association between multidisciplinary care and survival for elderly patients with chronic kidney disease. J Am Soc Nephrol 2007; 18: 993–999. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
