

Bedside calculation of mechanical power during volume- and pressure-controlled mechanical ventilation
- PMID: 32653011
- PMCID: PMC7351639
- DOI: 10.1186/s13054-020-03116-w
Bedside calculation of mechanical power during volume- and pressure-controlled mechanical ventilation
Abstract
Background: Mechanical power (MP) is the energy delivered to the respiratory system over time during mechanical ventilation. Our aim was to compare the currently available methods to calculate MP during volume- and pressure-controlled ventilation, comparing different equations with the geometric reference method, to understand whether the easier to use surrogate formulas were suitable for the everyday clinical practice. This would warrant a more widespread use of mechanical power to promote lung protection.
Methods: Forty respiratory failure patients, sedated and paralyzed for clinical reasons, were ventilated in volume-controlled ventilation, at two inspiratory flows (30 and 60 L/min), and pressure-controlled ventilation with a similar tidal volume. Mechanical power was computed both with the geometric method, as the area between the inspiratory limb of the airway pressure and the volume, and with two algebraic methods, a comprehensive and a surrogate formula.
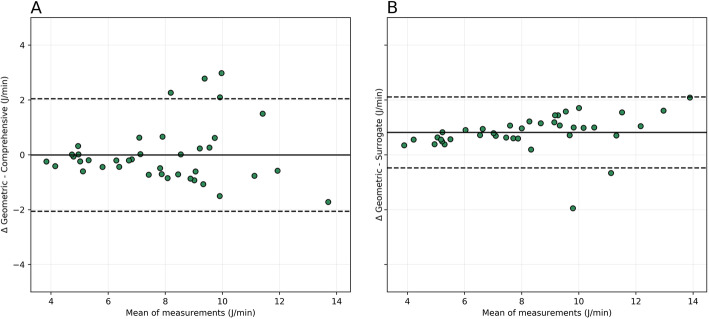
Results: The bias between the MP computed by the geometric method and by the comprehensive algebraic method during volume-controlled ventilation was respectively 0.053 (0.77, - 0.81) J/min and - 0.4 (0.70, - 1.50) J/min at low and high flows (r2 = 0.96 and 0.97, p < 0.01). The MP measured and computed by the two methods were highly correlated (r2 = 0.95 and 0.94, p < 0.01) with a bias of - 0.0074 (0.91, - 0.93) and - 1.0 (0.45, - 2.52) J/min at high-low flows. During pressure-controlled ventilation, the bias between the MP measured and the one calculated with the comprehensive and simplified methods was correlated (r2 = 0.81, 0.94, p < 0.01) with mean differences of - 0.001 (2.05, - 2.05) and - 0.81 (2.11, - 0.48) J/min.
Conclusions: Both for volume-controlled and pressure-controlled ventilation, the surrogate formulas approximate the reference method well enough to warrant their use in the everyday clinical practice. Given that these formulas require nothing more than the variables already displayed by the intensive care ventilator, a more widespread use of mechanical power should be encouraged to promote lung protection against ventilator-induced lung injury.
Keywords: Acute respiratory distress syndrome; Acute respiratory failure; Driving pressure; Lung protection; Lung protective ventilation; Mechanical power; Mechanical ventilation; Respiratory failure; Respiratory rate; Ventilator-induced lung injury.
Conflict of interest statement
None to disclose.
Figures


References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, Adhikari NKJ, Amato MBP, Branson R, Brower RG, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
