

COVID-19 and the Global Impact on Colorectal Practice and Surgery
- PMID: 32653470
- PMCID: PMC7276135
- DOI: 10.1016/j.clcc.2020.05.011
COVID-19 and the Global Impact on Colorectal Practice and Surgery
Abstract
Background: The novel severe acute respiratory syndrome coronavirus 2 virus that emerged in December 2019 causing coronavirus disease 2019 (COVID-19) has led to the sudden national reorganization of health care systems and changes in the delivery of health care globally. The purpose of our study was to use a survey to assess the global effects of COVID-19 on colorectal practice and surgery.
Materials and methods: A panel of International Society of University Colon and Rectal Surgeons (ISUCRS) selected 22 questions, which were included in the questionnaire. The questionnaire was distributed electronically to ISUCRS fellows and other surgeons included in the ISUCRS database and was advertised on social media sites. The questionnaire remained open from April 16 to 28, 2020.
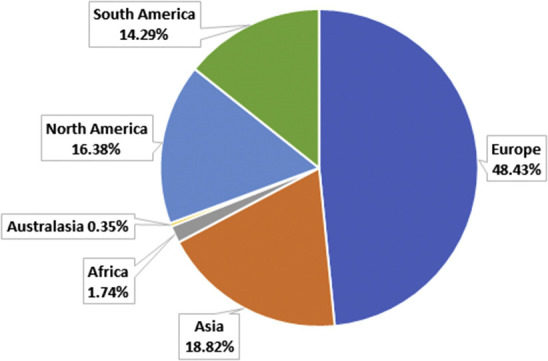
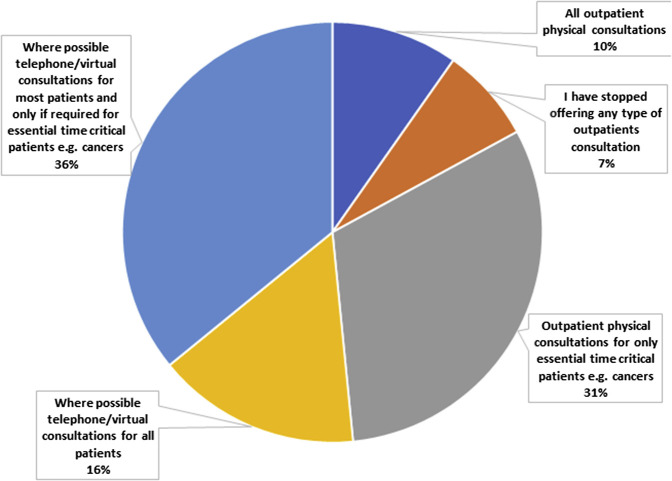
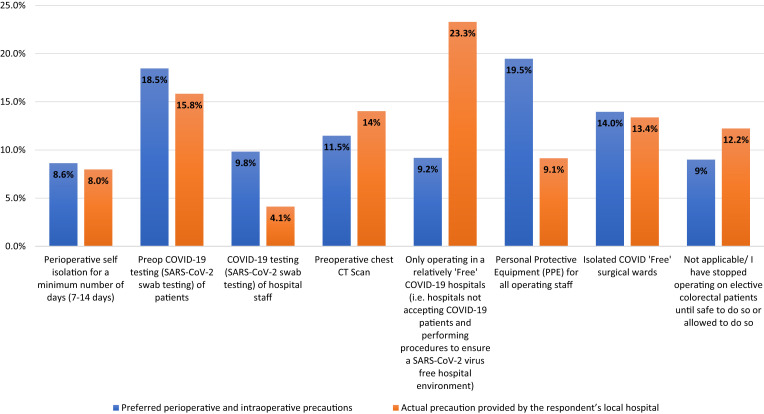
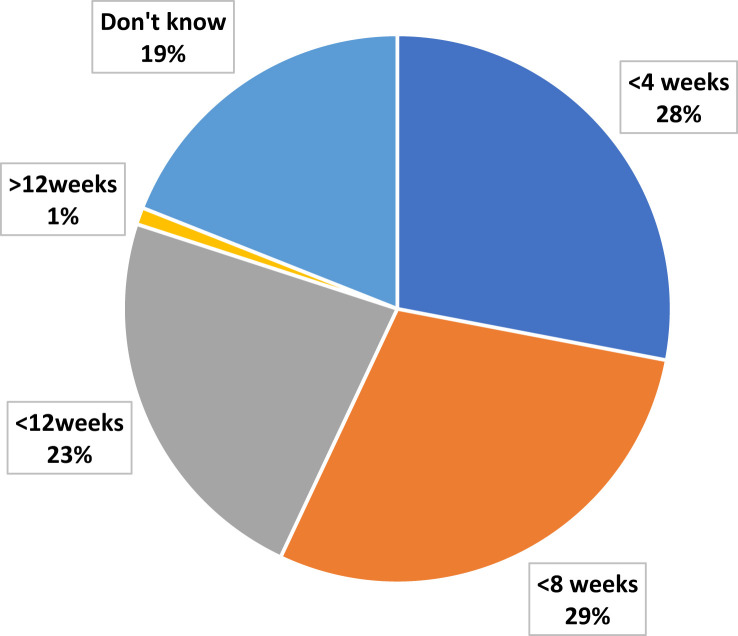
Results: A total of 287 surgeons completed the survey. Of the 287 respondents, 90% were colorectal specialists or general surgeons with an interest in colorectal disease. COVID-19 had affected the practice of 96% of the surgeons, and 52% were now using telemedicine. Also, 66% reported that elective colorectal cancer surgery could proceed but with perioperative precautions. Of the 287 respondents, 19.5% reported that the use of personal protective equipment was the most important perioperative precaution. However, personal protective equipment was only provided by 9.1% of hospitals. In addition, 64% of surgeons were offering minimally invasive surgery. However, 44% reported that enough information was not available regarding the safety of the loss of intra-abdominal carbon dioxide gas during the COVID-19 pandemic. Finally, 61% of the surgeons were prepared to defer elective colorectal cancer surgery, with 29% willing to defer for ≤ 8 weeks.
Conclusion: The results from our survey have demonstrated that, globally, COVID-19 has affected the ability of colorectal surgeons to offer care to their patients. We have also discussed suggestions for various practical adaptation strategies for use during the recovery period.
Keywords: Colorectal disease; Colorectal surgery; Guidance; SARS-CoV-2; Survey.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
