

Ixazomib for Chronic Graft-versus-Host Disease Prophylaxis following Allogeneic Hematopoietic Cell Transplantation
- PMID: 32653622
- PMCID: PMC7571859
- DOI: 10.1016/j.bbmt.2020.07.005
Ixazomib for Chronic Graft-versus-Host Disease Prophylaxis following Allogeneic Hematopoietic Cell Transplantation
Erratum in
-
Corrigendum to 'Ixazomib for chronic Graft-Versus-Host Disease prophylaxis following allogeneic hematopoietic cell transplantation' [Biology of Blood and Marrow Transplantation 26/10 (2020) 1876-1885].Transplant Cell Ther. 2022 Oct;28(10):717. doi: 10.1016/j.jtct.2021.01.005. Epub 2021 Jan 10. Transplant Cell Ther. 2022. PMID: 36202527 No abstract available.
Abstract
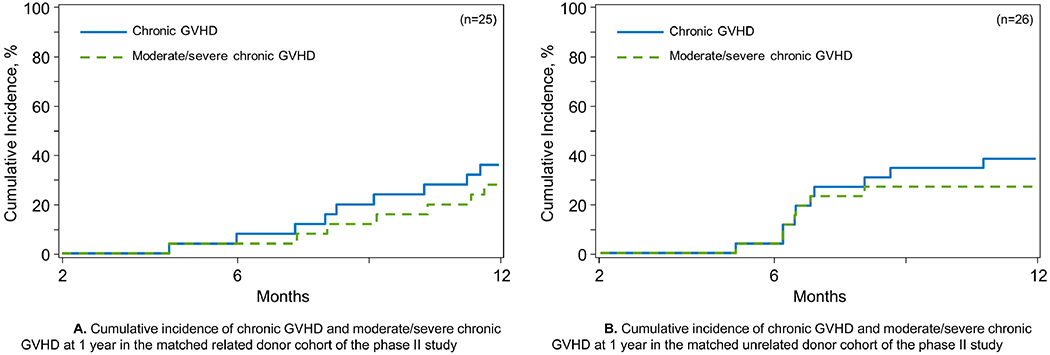
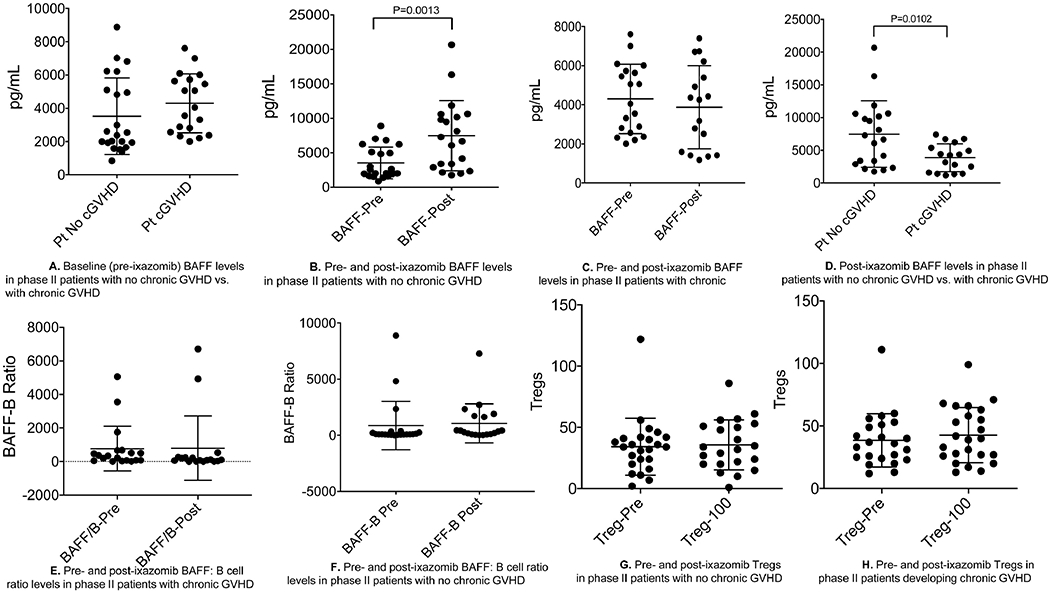
Chronic graft-versus-host disease (cGVHD) is major cause of morbidity and mortality following allogeneic hematopoietic cell transplantation (HCT). Ixazomib is an oral, second-generation, proteasome inhibitor that has been shown in preclinical models to prevent GVHD. We conducted a phase I/II trial in 57 patients to evaluate the safety and efficacy of ixazomib administration for cGVHD prophylaxis in patients undergoing allogeneic HCT. Oral ixazomib was administered on a weekly basis for a total of 4 doses, beginning days +60 through +90, to recipients of matched related donor (MRD, n = 25) or matched unrelated donor (MUD, n = 26) allogeneic HCT in phase II portion of the study, once the recommended phase II dose of 4 mg was identified in phase I (n = 6). All patients received peripheral blood graft and standard GVHD prophylaxis of tacrolimus and methotrexate. Ixazomib administration was safe and well tolerated, with thrombocytopenia, leukopenia, gastrointestinal complaints, and fatigue the most common adverse events (>10%). In phase II (n = 51), the cumulative incidence of cGVHD at 1 year was 36% (95% confidence interval [CI], 19% to 54%) in the MRD cohort and 39% (95% CI, 21% to 56%) in the MUD cohort. One-year cumulative incidence of nonrelapse mortality (NRM) and relapse was 0% and 20% (95% CI, 8% to 36%) in the MRD cohort, respectively. In the MUD cohort, the respective NRM and relapse rates were 4% (0% to 16%) and 34% (17% to 52%). The outcomes on the study were compared post hoc with contemporaneous matched Center for International Blood and Marrow Transplant Research (CIBMTR) controls. This post hoc analysis showed no significant improvement in cGVHD rates in both the MRD (hazard ratio [HR] = 0.85, P = .64) or MUD cohorts (HR = 0.68, P = .26) on the study compared with CIBMTR controls. B cell activating factor plasma levels were significantly higher after ixazomib dosing in those who remained cGVHD free compared with those developed cGVHD. This study shows that the novel strategy of short-course oral ixazomib following allogeneic HCT is safe but did not demonstrate significant improvement in cGVHD incidence in recipients of MRD and MUD transplantation compared with matched CIBMTR controls. This study is registered at www.clinicaltrials.gov as NCT02250300.
Keywords: Allogeneic hematopoietic cell transplantation; Graft-versus-host disease; Ixazomib.
Copyright © 2020 American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Arai S, Arora M, Wang T, et al. : Increasing incidence of chronic graft-versus-host disease in allogeneic transplantation: a report from the Center for International Blood and Marrow Transplant Research. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation 21:266–274, 2015 - PMC - PubMed
-
- Antin JH, Kim HT, Cutler C, et al. : Sirolimus, tacrolimus, and low-dose methotrexate for graft-versus-host disease prophylaxis in mismatched related donor or unrelated donor transplantation. Blood 102:1601–1605, 2003 - PubMed
-
- Nash RA, Antin JH, Karanes C, et al. : Phase 3 study comparing methotrexate and tacrolimus with methotrexate and cyclosporine for prophylaxis of acute graft-versus-host disease after marrow transplantation from unrelated donors. Blood 96:2062–8, 2000 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
