

Ultrasound of scrotal and penile emergency: how, why and when
- PMID: 32654040
- PMCID: PMC8137766
- DOI: 10.1007/s40477-020-00500-8
Ultrasound of scrotal and penile emergency: how, why and when
Abstract
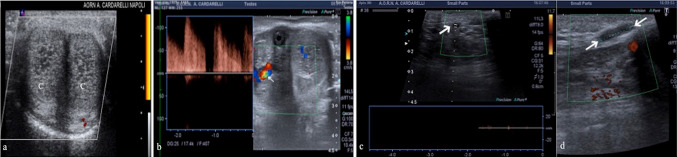
High-resolution ultrasound is the most common imaging technique used to supplement the physical examination of scrotum and penis with great accuracy in assisting the diagnosis of the various pathologies of male genital system, with the highest diagnostic potential in emergency conditions. Technical advancements in real-time high-resolution, color flow Doppler sonography and contrast enhanced ultrasonography (CEUS) have led to an increase in the clinical applications of scrotal and penile sonography. In this pictorial review we focus on common and uncommon male genitalia emergency with special emphasis on the role of ultrasound assessment and its specific findings to improve diagnostic accuracy.
Keywords: CEUS; Color-doppler; Emergency; Penis; Testis; Ultrasound.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures







References
-
- Gorman B. The scrotum. In: Rumack CM, editor. Diagnostic ultrasound. 4. Philadelphia: Elsevier; 2011. pp. 840–877.
-
- Pozniak MA, Allan P (2014) Clinical Doppler Ultrasound—ClinicalKey. In: Churchill Livingstone Elsevier 3rd edn, pp261–294
-
- Dogra VS, Bhatt S, Rubens DJ. Sonographic evaluation of testicular torsion. Ultrasound Clin. 2006;1(1):55–66. doi: 10.1016/j.cult.2005.09.006. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
