

Telling friend from foe in emergency vertigo and dizziness: does season and daytime of presentation help in the differential diagnosis?
- PMID: 32654062
- PMCID: PMC7718175
- DOI: 10.1007/s00415-020-10019-x
Telling friend from foe in emergency vertigo and dizziness: does season and daytime of presentation help in the differential diagnosis?
Abstract
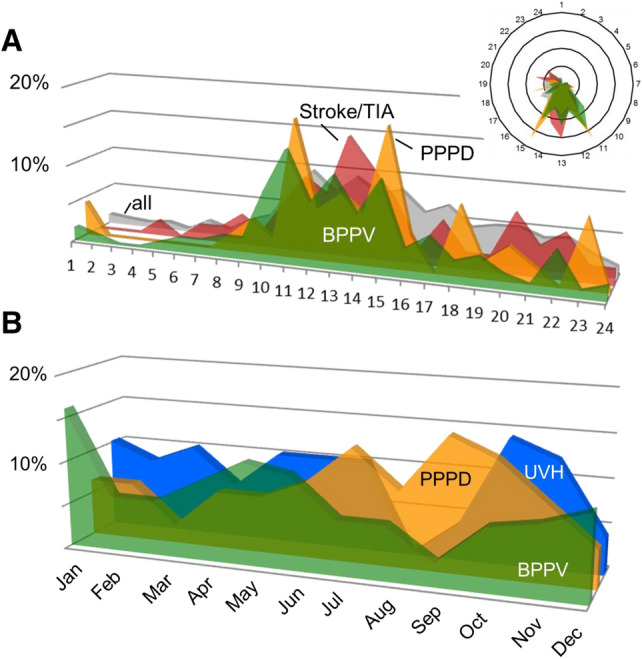
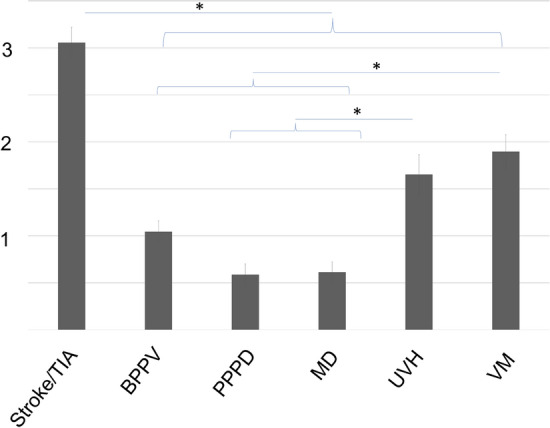
Distinguishing between serious (e.g., stroke) and benign (e.g., benign paroxysmal positional vertigo, BPPV) disorders remains challenging in emergency consultations for vertigo and dizziness (VD). A number of clues from patient history and clinical examination, including several diagnostic index tests have been reported recently. The objective of the present study was to analyze frequency and distribution patterns of specific vestibular and non-vestibular diagnoses in an interdisciplinary university emergency room (ER), including data on daytime and season of presentation. A retrospective chart analysis of all patients seen in a one-year period was performed. In the ER 4.23% of all patients presented with VD (818 out of 19,345). The most frequent-specific diagnoses were BPPV (19.9%), stroke/transient ischemic attack (12.5%), acute unilateral vestibulopathy/vestibular neuritis (UVH; 8.3%), and functional VD (8.3%). Irrespective of the diagnosis, the majority of patients presented to the ER between 8 a.m. and 4 p.m. There are, however, seasonal differences. BPPV was most prevalent in December/January and rare in September. UVH was most often seen in October/November; absolute and relative numbers were lowest in August. Finally, functional/psychogenic VD was common in summer and autumn with highest numbers in September/October and lowest numbers in March. In summary, daytime of presentation did not distinguish between diagnoses as most patients presented during normal working hours. Seasonal presentation revealed interesting fluctuations. The UVH peak in autumn supports the viral origin of the condition (vestibular neuritis). The BPPV peak in winter might be related to reduced physical activity and low vitamin D. However, it is likely that multiple factors contribute to the fluctuations that have to be disentangled in further studies.
Keywords: Benign paroxysmal positional vertigo; Dizziness; Emergency room; Stroke; Vertigo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
