

Endothelium-Macrophage Crosstalk Mediates Blood-Brain Barrier Dysfunction in Hypertension
- PMID: 32654560
- PMCID: PMC7429290
- DOI: 10.1161/HYPERTENSIONAHA.120.15581
Endothelium-Macrophage Crosstalk Mediates Blood-Brain Barrier Dysfunction in Hypertension
Abstract
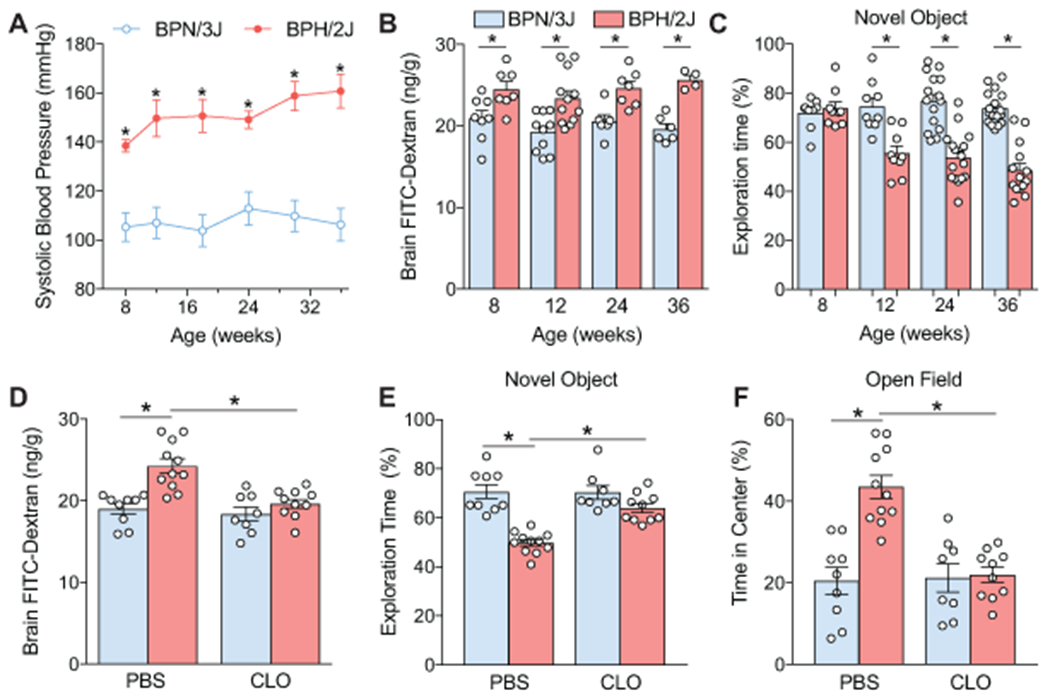
Hypertension is a leading cause of stroke and dementia, effects attributed to disrupting delivery of blood flow to the brain. Hypertension also alters the blood-brain barrier (BBB), a critical component of brain health. Although endothelial cells are ultimately responsible for the BBB, the development and maintenance of the barrier properties depend on the interaction with other vascular-associated cells. However, it remains unclear if BBB disruption in hypertension requires cooperative interaction with other cells. Perivascular macrophages (PVM), innate immune cells closely associated with cerebral microvessels, have emerged as major contributors to neurovascular dysfunction. Using 2-photon microscopy in vivo and electron microscopy in a mouse model of Ang II (angiotensin II) hypertension, we found that the vascular segments most susceptible to increased BBB permeability are arterioles and venules >10 µm and not capillaries. Brain macrophage depletion with clodronate attenuates, but does not abolish, the increased BBB permeability in these arterioles where PVM are located. Deletion of AT1R (Ang II type-1 receptors) in PVM using bone marrow chimeras partially attenuated the BBB dysfunction through the free radical-producing enzyme Nox2. In contrast, downregulation of AT1R in cerebral endothelial cells using a viral gene transfer-based approach prevented the BBB disruption completely. The results indicate that while endothelial AT1R, mainly in arterioles and venules, initiate the BBB disruption in hypertension, PVM are required for the full expression of the dysfunction. The findings unveil a previously unappreciated contribution of resident brain macrophages to increased BBB permeability of hypertension and identify PVM as a putative therapeutic target in diseases associated with BBB dysfunction.
Keywords: angiotensin II; arterioles; cerebrovascular circulation; cognitive dysfunction.
Conflict of interest statement
DISCLOSURES
CI serves on the strategic advisory board of Broadview Ventures. The other authors have no conflicts to disclose.
Figures





References
-
- WHO. A global brief on hypertension : Silent killer, global public health crisis. World health organization. 2013
-
- Forouzanfar MH, Liu P, Roth GA, Ng M, Biryukov S, Marczak L, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mmHg, 1990-2015. Jama. 2017;317:165–182 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
