

Diabetes and Hepatocellular Carcinoma: Incidence Trends and Impact of Liver Disease Etiology
- PMID: 32655232
- PMCID: PMC7335702
- DOI: 10.1016/j.jceh.2019.11.004
Diabetes and Hepatocellular Carcinoma: Incidence Trends and Impact of Liver Disease Etiology
Abstract
Background/aims: Hepatocellular carcinoma (HCC) remains the leading cause of cancer-related death among patients with type 2 diabetes mellitus (T2DM). We aimed to assess the independent role of T2DM on HCC risk among patients with different liver disease etiologies.
Methods: We analyzed the United Network for Organ Sharing database of all adults registered for liver transplantation (LT) between February 27, 2002 and December 31, 2017. For initial analyses, patients were divided into four groups: nonalcoholic steatohepatitis (NASH) and all other etiologies with or without T2DM. For additional analyses, we divided them based on underlying etiology. Logistic regression was used to evaluate the impact of T2DM with NASH and other etiologies on HCC risk.
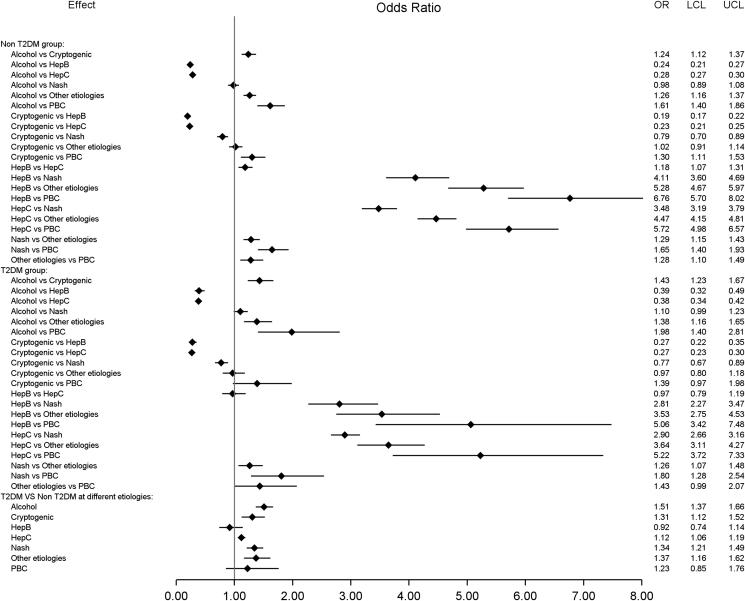
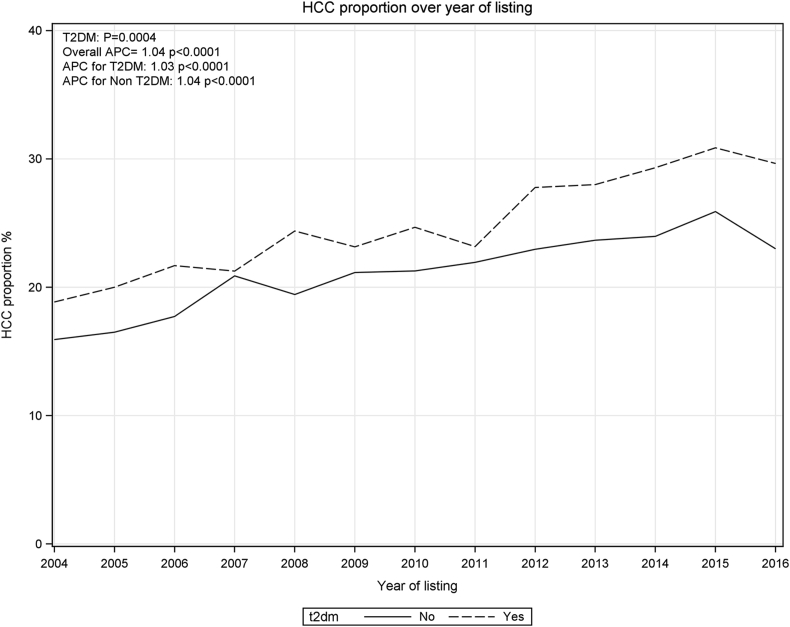
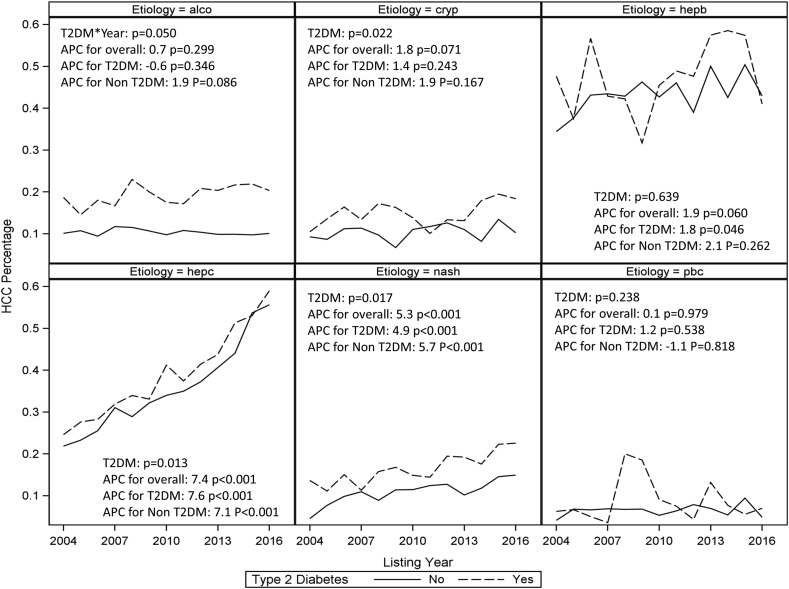
Results: Overall, 24,149 (21.6%) of the listed patients had HCC. Of those, 23.9% had T2DM. When compared with nondiabetics, patient with NASH and T2DM had the highest risk of HCC (odds ratio [OR] 1.68; 95% confidence interval [CI] 1.52-1.86), followed by patients with other etiologies and diabetes. After adjusting for other risk factors, these associations remained unchanged. Registrants with T2DM and NASH, cryptogenic cirrhosis, hepatitis C, and alcoholic liver disease were at higher risk of HCC than those without diabetes, but in patients with chronic hepatitis B or primary biliary cholangitis, diabetes did not increase the HCC risk. Between 2004 and 2016, the annual percentage change of HCC incidence increased for all patients with NASH and hepatitis C regardless of their diabetes status. For those with hepatitis B, this trend was significant only for diabetics.
Conclusions: The additive risk of T2DM for HCC development was highest in patients with NASH. HCC risk may vary depending on the underlying etiology.
Keywords: ALD, alcoholic liver disease; APC, annual percentage change; CI, confidence interval; HBV, hepatitis B virus; HCC incidence; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; LT, liver transplantation; MELD, Model for End-Stage Liver Disease; NAFLD, nonalcoholic liver disease; NASH, nonalcoholic steatohepatitis; OR, odds ratio; PBC, primary biliary cholangitis; T2DM, type 2 diabetes mellitus; UNOS; UNOS, United Network for Organ Sharing; fatty liver; liver cancer.
© 2019 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors have none to declare.
Figures
References
-
- Bertuccio P., Turati F., Carioli G. Global trends and predictions in hepatocellular carcinoma mortality. J Hepatol. 2017;67:302–309. - PubMed
-
- Younossi Z., Stepanova M., Ong J.P. Nonalcoholic steatohepatitis is the fastest growing cause of hepatocellular carcinoma in liver transplant candidates. Clin Gastroenterol Hepatol. 2019;17:748–755 e3. - PubMed
LinkOut - more resources
Full Text Sources
