

Full endoscopic cervical spine surgery
- PMID: 32656375
- PMCID: PMC7340839
- DOI: 10.21037/jss.2019.10.15
Full endoscopic cervical spine surgery
Abstract
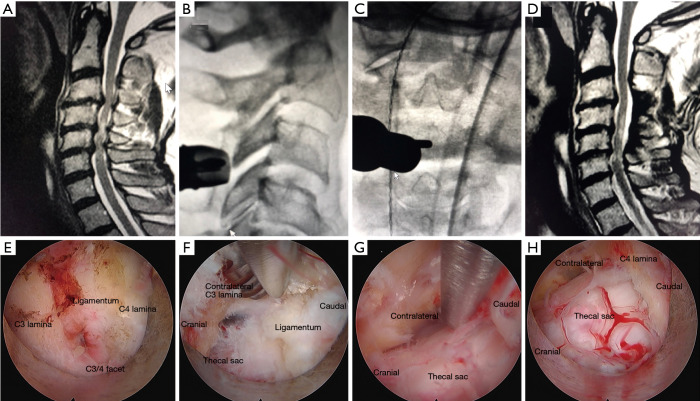
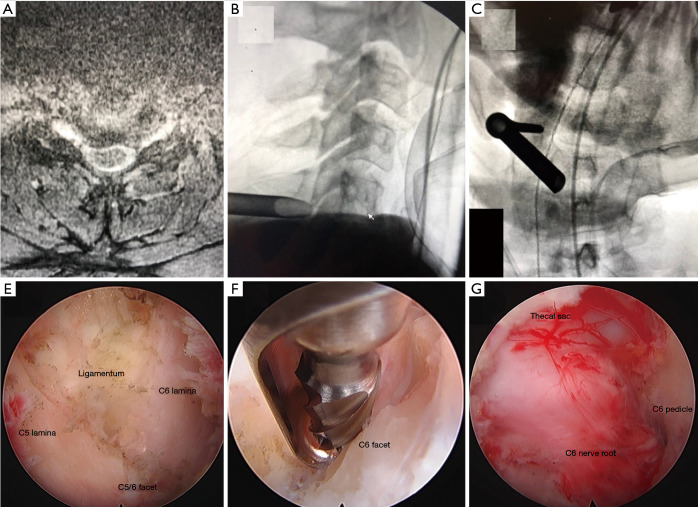
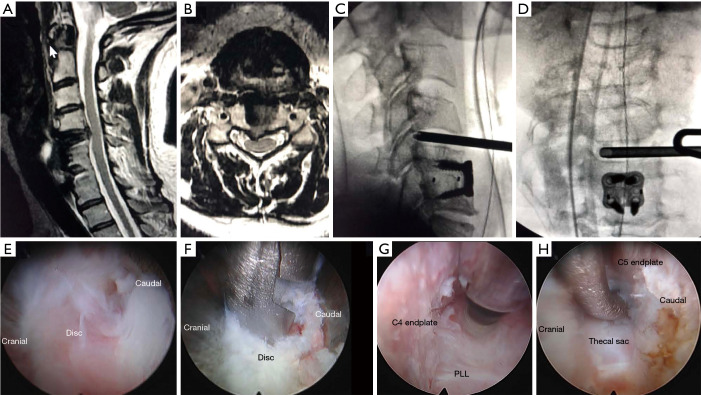
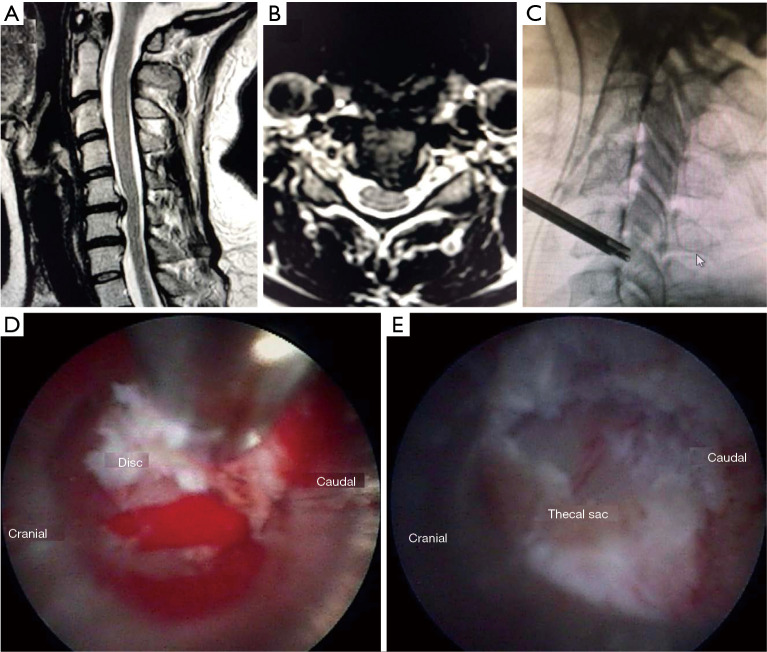
Background: The authors present 4 techniques for fully-endoscopic cervical spine surgery with accompanying case series: (I) posterior cervical unilateral laminectomy and bilateral decompression, (II) posterior cervical foraminotomy (PCF), (III) anterior cervical discectomy, and (IV) anterior transcorporeal discectomy.
Methods: We retrospectively reviewed fully endoscopic cervical spine surgery cases at one high-volume endoscopic center in the United States and present clinical data extracted from endoscopic spine surgery performed over a 6-year period with a minimum clinical follow up of 1 year.
Results: A series of 114 patients who underwent fully endoscopic cervical spine surgery between 2012 and 2018 is presented. Clinical results and technical data are presented.
Conclusions: Fully endoscopic cervical spine surgery is an emerging surgical technique for addressing cervical radiculopathy and myelopathy through a minimally invasive approach.
Keywords: Endoscopic spine surgery; cervical radiculopathy; minimally-invasive; myelopathy.
2020 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jss.2019.10.15). The series “Full-endoscopic Spine Surgery” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources