

Anticoagulation Timing in Cardioembolic Stroke and Recurrent Event Risk
- PMID: 32656768
- PMCID: PMC8259451
- DOI: 10.1002/ana.25844
Anticoagulation Timing in Cardioembolic Stroke and Recurrent Event Risk
Abstract
Objective: Guidelines recommend initiating anticoagulation within 4 to 14 days after cardioembolic stroke. Data supporting this did not account for key factors potentially affecting the decision to initiate anticoagulation, such as infarct size, hemorrhagic transformation, or high-risk features on echocardiography.
Methods: We pooled data from stroke registries of 8 comprehensive stroke centers across the United States. We included consecutive patients admitted with ischemic stroke and atrial fibrillation. The primary predictor was timing of initiating anticoagulation (0-3 days, 4-14 days, or >14 days), and outcomes were recurrent stroke/transient ischemic attack/systemic embolism, symptomatic intracerebral hemorrhage (sICH), and major extracranial hemorrhage (ECH) within 90 days.
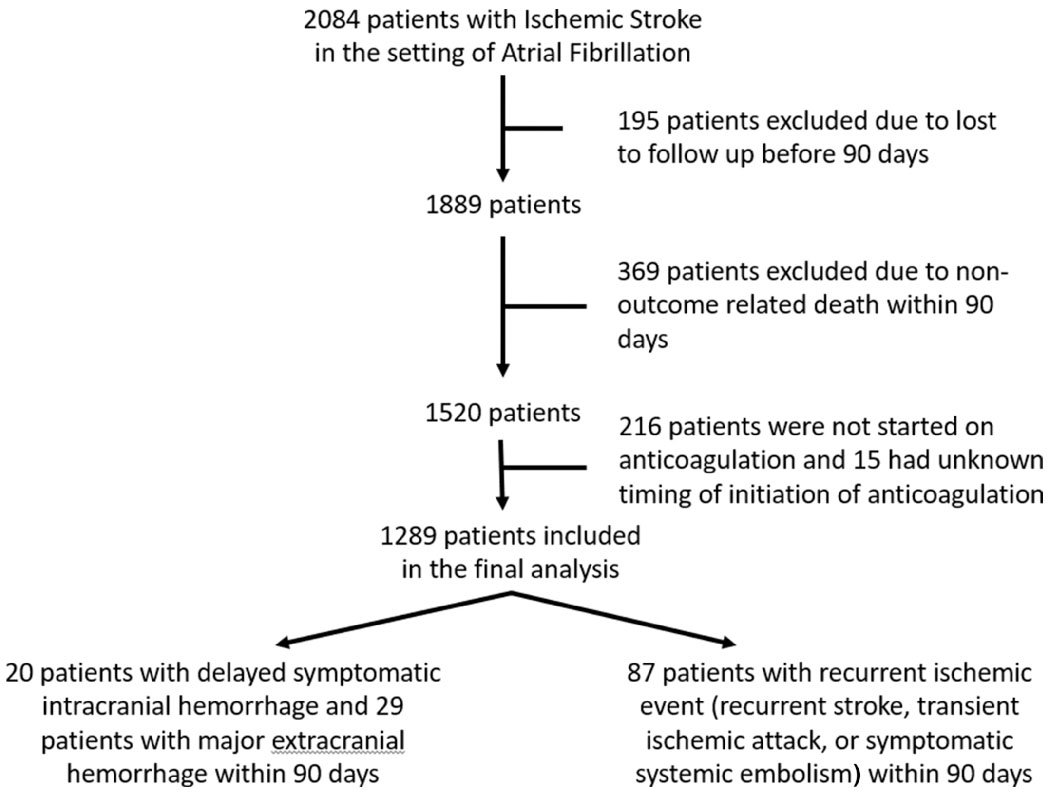
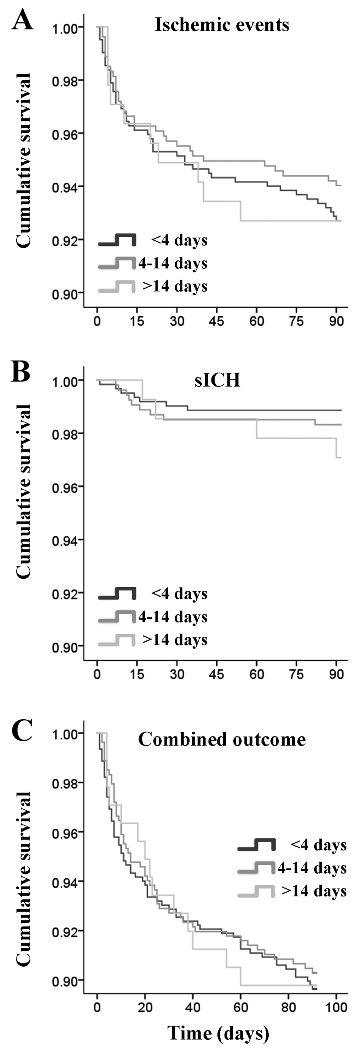
Results: Among 2,084 patients, 1,289 met the inclusion criteria. The combined endpoint occurred in 10.1% (n = 130) subjects (87 ischemic events, 20 sICH, and 29 ECH). Overall, there was no significant difference in the composite endpoint between the 3 groups (0-3 days: 10.3%, 64/617; 4-14 days: 9.7%, 52/535; >14 days: 10.2%, 14/137; p = 0.933). In adjusted models, patients started on anticoagulation between 4 and 14 days did not have a lower rate of sICH (vs 0-3 days; odds ratio [OR] = 1.49, 95% confidence interval [CI] = 0.50-4.43), nor did they have a lower rate of recurrent ischemic events (vs >14 days; OR = 0.76, 95% CI = 0.36-1.62, p = 0.482).
Interpretation: In this multicenter real-world cohort, the recommended (4-14 days) time frame to start oral anticoagulation was not associated with reduced ischemic and hemorrhagic outcomes. Randomized trials are required to determine the optimal timing of anticoagulation initiation. ANN NEUROL 2020;88:807-816.
© 2020 American Neurological Association.
Conflict of interest statement
Potential conflict of interest: all authors have no relevant conflict of interest
Figures
References
-
- Sacchetti DC, Furie KL, Yaghi S. Cardioembolic stroke: Mechanisms and therapeutics. Seminars in neurology. 2017;37:326–338 - PubMed
-
- Low molecular weight heparinoid, org 10172 (danaparoid), and outcome after acute ischemic stroke: A randomized controlled trial. The publications committee for the trial of org 10172 in acute stroke treatment (toast) investigators. Jama. 1998;279:1265–1272 - PubMed
-
- Berge E, Abdelnoor M, Nakstad PH, Sandset PM. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: A double-blind randomised study. Haest study group. Heparin in acute embolic stroke trial. Lancet (London, England). 2000;355:1205–1210 - PubMed
-
- The international stroke trial (ist): A randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. International stroke trial collaborative group. Lancet (London, England). 1997;349:1569–1581 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
