

Stereotactic Cardiac Radiation to Control Ventricular Tachycardia and Fibrillation Storm in a Patient with Apical Hypertrophic Cardiomyopathy at Burnout Stage: Case Report
- PMID: 32657082
- PMCID: PMC7358068
- DOI: 10.3346/jkms.2020.35.e200
Stereotactic Cardiac Radiation to Control Ventricular Tachycardia and Fibrillation Storm in a Patient with Apical Hypertrophic Cardiomyopathy at Burnout Stage: Case Report
Abstract
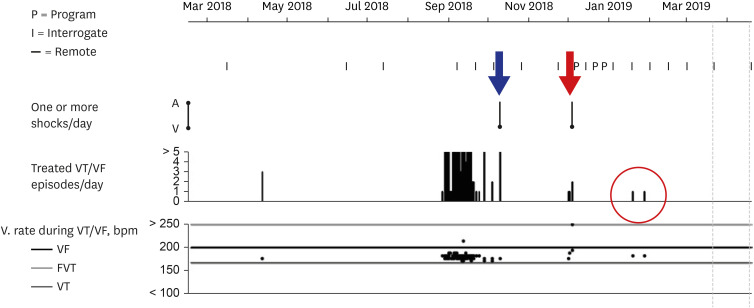
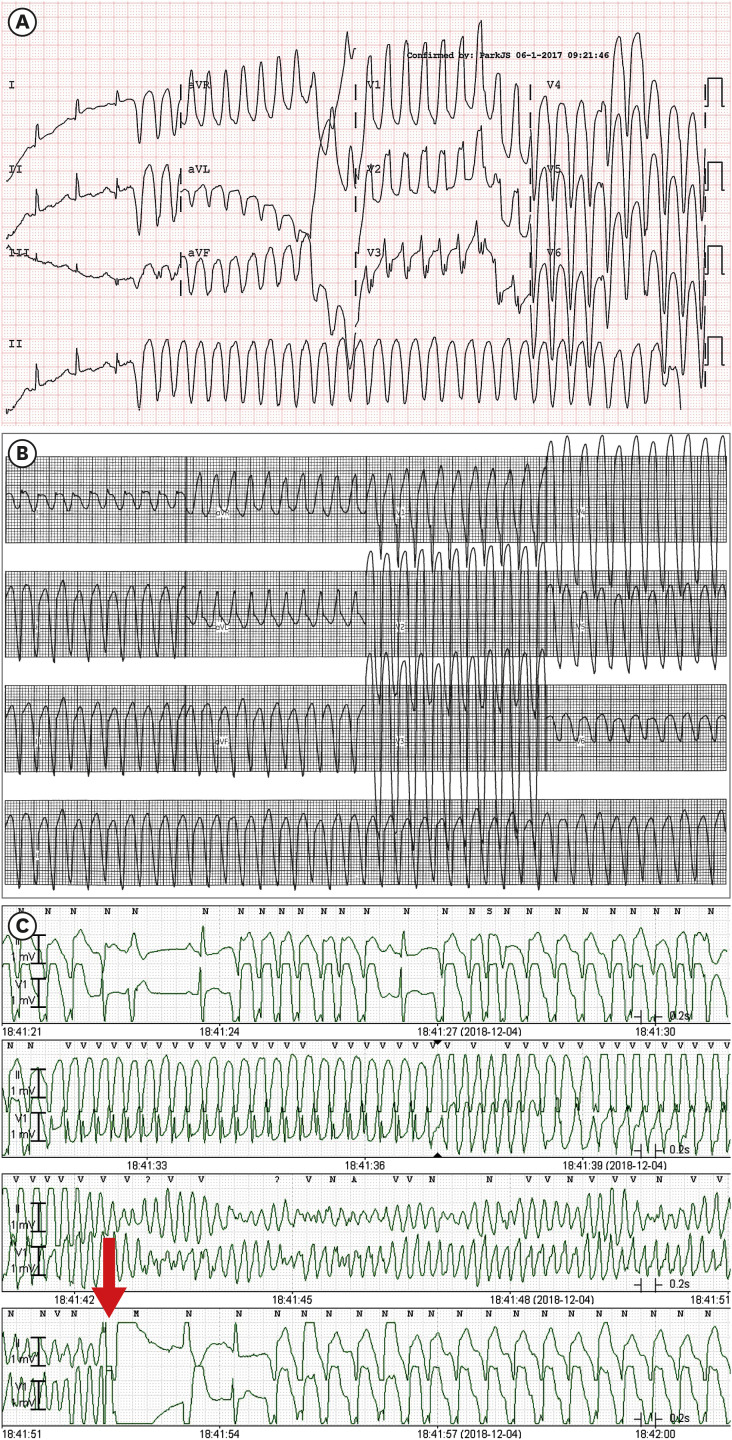
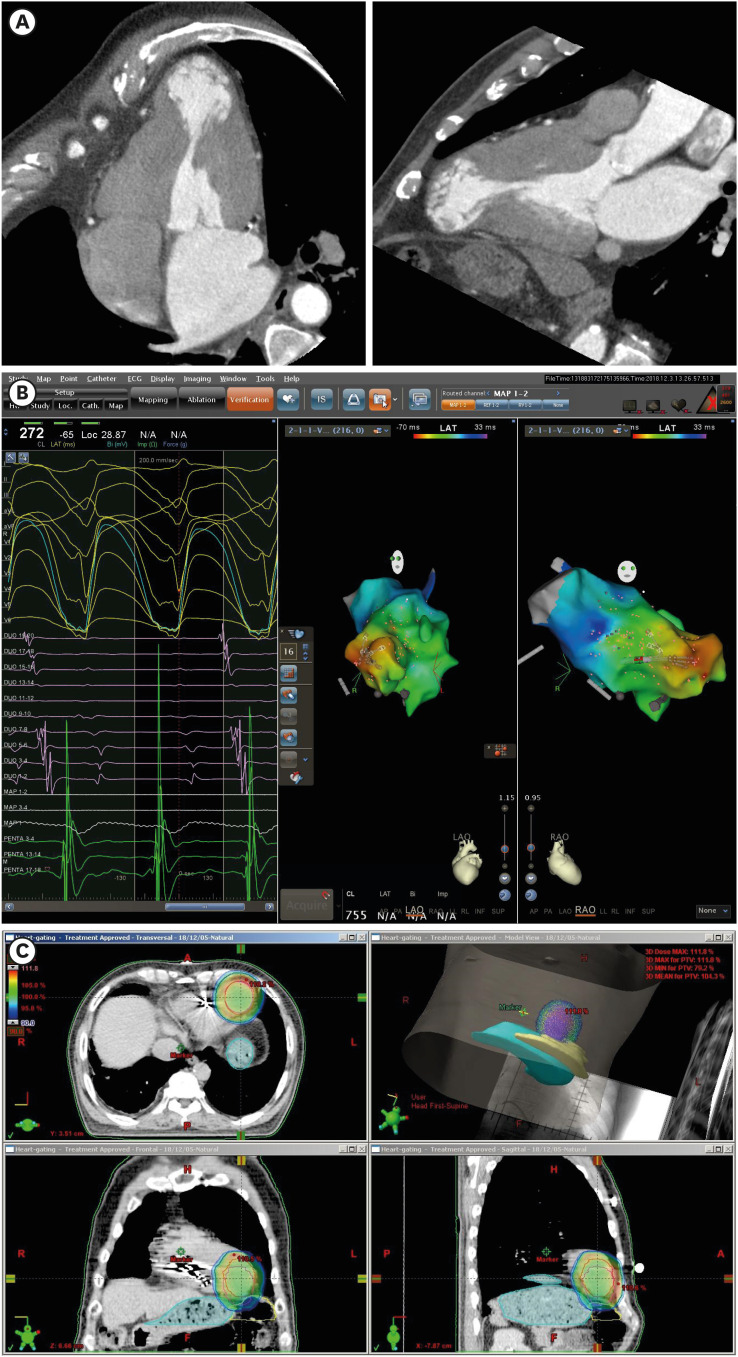
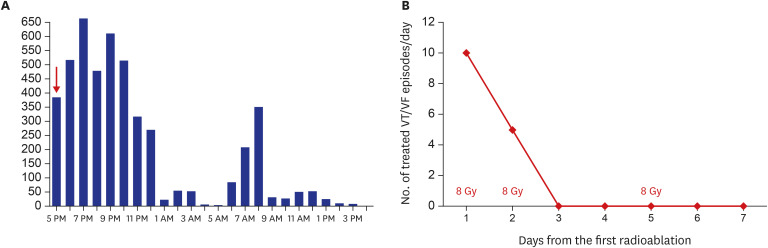
Stereotactic cardiac radiation for ablation (radioablation) of life-threatening ventricular arrhythmia was recently introduced into clinical practice. A 76-year-old male patient with apical hypertrophic cardiomyopathy at burnout stage, who received defibrillator implantation for the secondary prevention of sudden arrhythmic death, was admitted for repeated defibrillator therapy. Radiofrequency catheter ablation was unsuccessful due to the induction of ventricular fibrillation (VF) and hemodynamically unstable sustained monomorphic ventricular tachycardia (VT). However, intracardiac activation mapping for the induced VT revealed the earliest ventricular activation at the apical aneurysm. Radioablation was performed to control VT and VF storm refractory to antiarrhythmic drug therapy. A total of 24 Gray was radiated, divided into three fractions around the apical aneurysm. The onset of electrical modulation was instantaneous and the antiarrhythmic effect was maintained for at least 6 months without significant radiation toxicities. This case suggests that radioablation may be considered as a rescue therapy for VT and VF storm refractory to other treatment modalities.
Keywords: Ablation; Cardiomyopathy; Radiation; Ventricular Tachycardia.
© 2020 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Comment in
-
Letter to the Editor: Stereotactic Cardiac Radiation to Control Ventricular Tachycardia and Fibrillation Storm in a Patient with Apical Hypertrophic Cardiomyopathy at Burnout Stage: Case Report.J Korean Med Sci. 2020 Nov 9;35(43):e381. doi: 10.3346/jkms.2020.35.e381. J Korean Med Sci. 2020. PMID: 33169561 Free PMC article. No abstract available.
References
-
- Loo BW, Jr, Soltys SG, Wang L, Lo A, Fahimian BP, Iagaru A, et al. Stereotactic ablative radiotherapy for the treatment of refractory cardiac ventricular arrhythmia. Circ Arrhythm Electrophysiol. 2015;8(3):748–750. - PubMed
-
- Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Kavanagh B, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 2010;37(8):4078–4101. - PubMed
-
- Sharma A, Wong D, Weidlich G, Fogarty T, Jack A, Sumanaweera T, et al. Noninvasive stereotactic radiosurgery (CyberHeart) for creation of ablation lesions in the atrium. Heart Rhythm. 2010;7(6):802–810. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
