

The Neurofibromatoses
- PMID: 32657748
- PMCID: PMC7373809
- DOI: 10.3238/arztebl.2020.0354
The Neurofibromatoses
Abstract
Background: Neurofibromatosis of types 1 and 2 (NF1, NF2) and schwannomatosis are the diseases that make up the neurofibromatosis spectrum. With respective incidences of 1 in 3000, 1 in 33 000, and 1 in 60 000 births, they form part of the group of rare tumor-suppressor syndromes. They give rise to a greater tumor burden for the nervous system than any other type of neoplastic disease. New approaches to symptomatic treatment are emerging.
Methods: This review is based on articles retrieved by a selective literature search on the pathogenesis, diagnosis, and treatment of the neurofibromatoses.
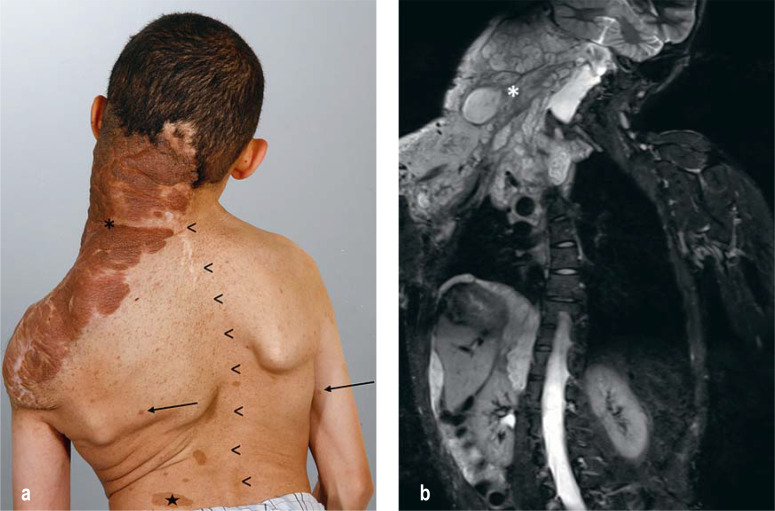
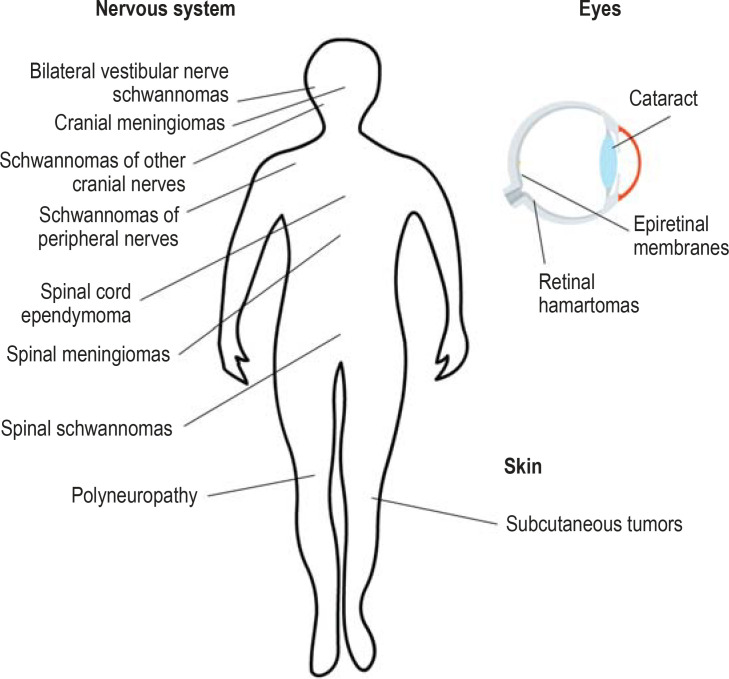
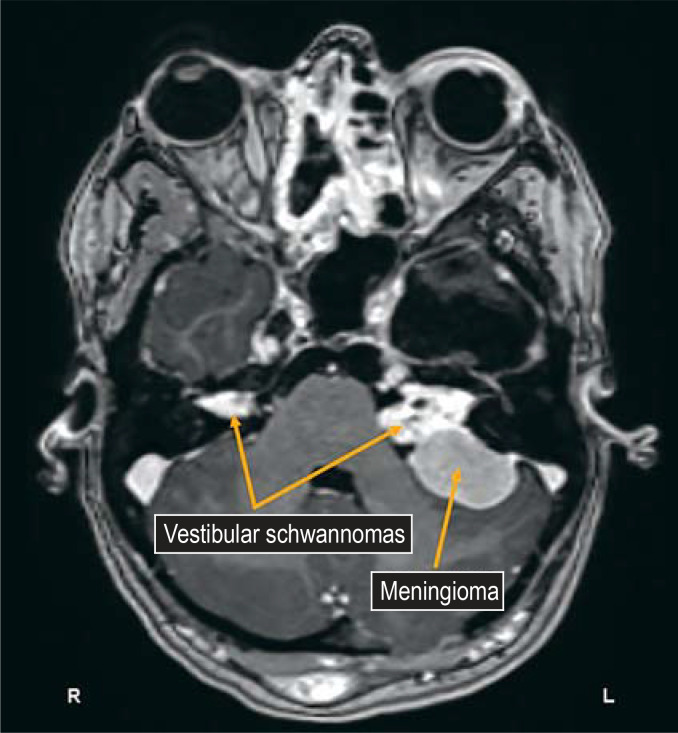
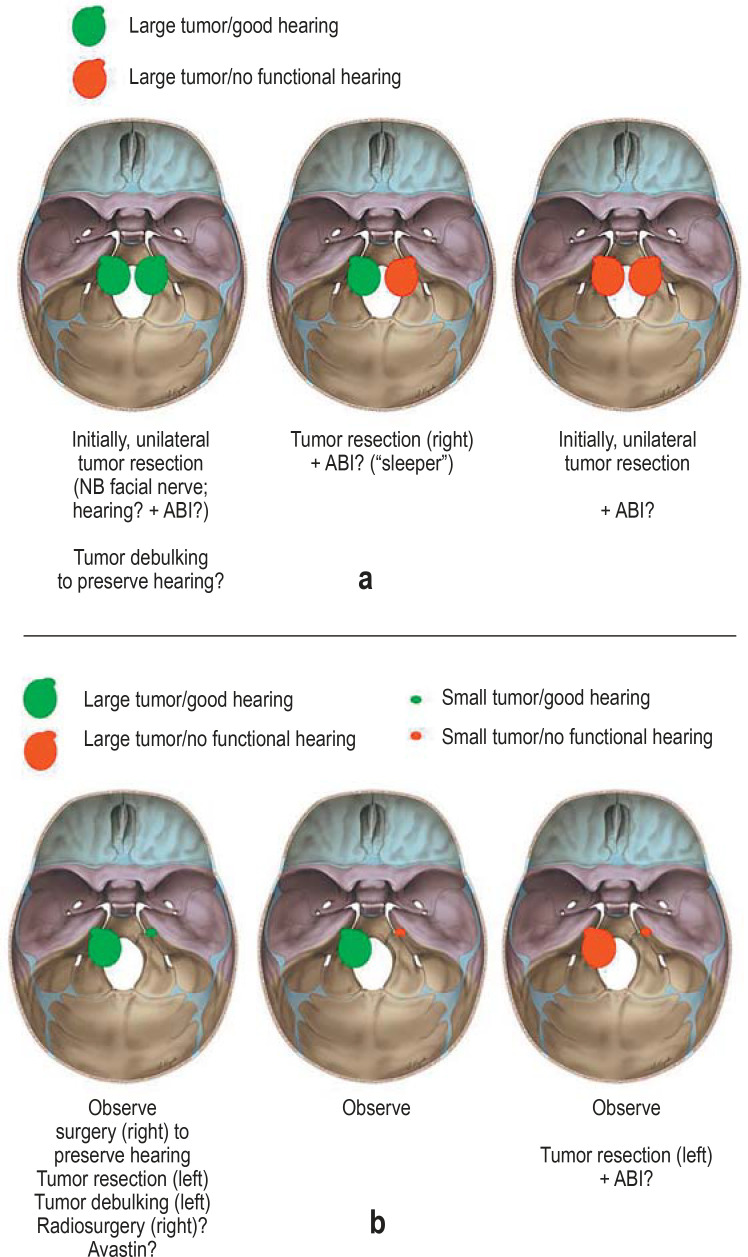
Results: NF1 and NF2 are monogenic diseases, while the genetics of schwannomatosis is complex. The three entities are clinically and pathophysiologically distinct. An important aspect of their tumor biology is the alternation of growth phases and growth pauses. Correlations between genotypes and phenotypes are variable, while new mutations and genetic mosaics are common. Ninety-nine percent of patients with NF1 have six or more café-au-lait spots by the age of 12 months; 90-95% of patients with NF2 develop bilateral vestibular schwannomas. In schwannomatosis, pain is the most prominent symptom; two-thirds of those affected develop spinal schwannomas. The severity and prognosis of these disorders are not closely correlated with the radiological findings; rather, neurologic deficits, malignant transformation, and psychosocial stress are of greater clinical importance. Advances in knowledge of pathophysiology have led to the development of targeted treatment approaches. Examples include the off-label treatment of vestibular schwannomas with bevacizumab and of plexiform neurofibromas with MEK inhibitors.
Conclusion: Patients with neurofibromatoses need individualized care. They should be treated in centers of expertise where interdisciplinary consultation is available and new types of pharmacotherapy can be provided.
Figures
Comment in
-
Screening: The Significance of Pheochromocytoma.Dtsch Arztebl Int. 2021 Jan 29;118(4):56. doi: 10.3238/arztebl.m2021.0042. Dtsch Arztebl Int. 2021. PMID: 33759746 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2021 Jan 29;118(4):56. doi: 10.3238/arztebl.m2021.0043. Dtsch Arztebl Int. 2021. PMID: 33759747 Free PMC article. No abstract available.
-
Urolithiasis/Endourology.J Urol. 2021 Nov;206(5):1321-1324. doi: 10.1097/JU.0000000000002151. Epub 2021 Aug 18. J Urol. 2021. PMID: 34406026 No abstract available.
References
-
- Hirbe AC, Gutmann DH. Neurofibromatosis type 1: a multidisciplinary approach to care. Lancet Neurol. 2014;13:834–843. - PubMed
-
- DeBella K, Szudek J, Friedman JM. Use of the national institutes of health criteria for diagnosis of neurofibromatosis 1 in children. Pediatrics. 2000;105:608–614. - PubMed
-
- Mautner V-F, Lindenau M, Kaufmann D. Klinik und Genetik der Neurofibromatose. Dtsch Arztebl. 1995;92:A1759–A1764.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous