

Association Between Plant and Animal Protein Intake and Overall and Cause-Specific Mortality
- PMID: 32658243
- PMCID: PMC7358979
- DOI: 10.1001/jamainternmed.2020.2790
Association Between Plant and Animal Protein Intake and Overall and Cause-Specific Mortality
Abstract
Importance: Although emphasis has recently been placed on the importance of high-protein diets to overall health, a comprehensive analysis of long-term cause-specific mortality in association with the intake of plant protein and animal protein has not been reported.
Objective: To examine the associations between overall mortality and cause-specific mortality and plant protein intake.
Design, setting, and participants: This prospective cohort study analyzed data from 416 104 men and women in the US National Institutes of Health-AARP Diet and Health Study from 1995 to 2011. Data were analyzed from October 2018 through April 2020.
Exposures: Validated baseline food frequency questionnaire dietary information, including intake of plant protein and animal protein.
Main outcomes and measures: Hazard ratios and 16-year absolute risk differences for overall mortality and cause-specific mortality.
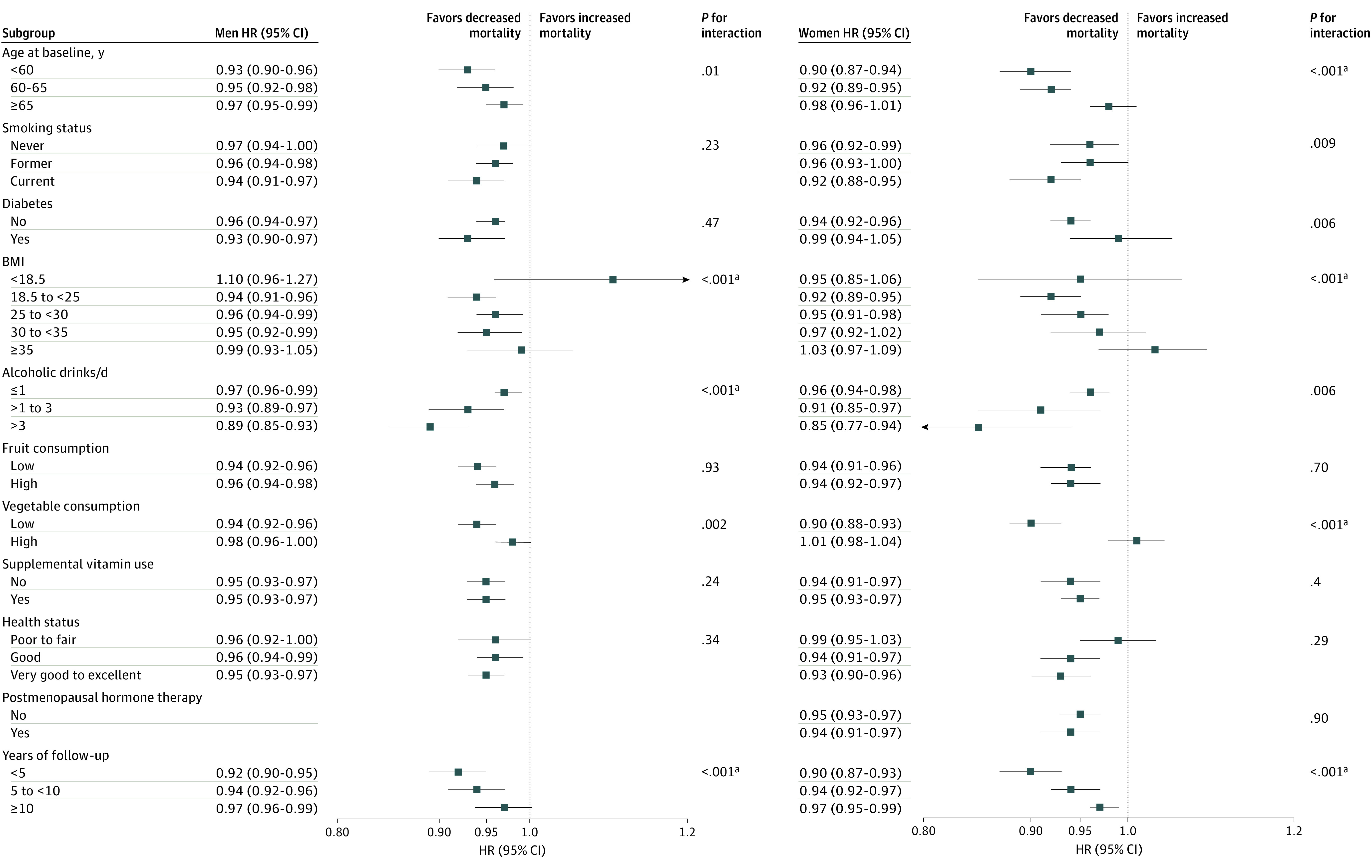
Results: The final analytic cohort included 237 036 men (57%) and 179 068 women. Their overall median (SD) ages were 62.2 (5.4) years for men and 62.0 (5.4) years for women. Based on 6 009 748 person-years of observation, 77 614 deaths (18.7%; 49 297 men and 28 317 women) were analyzed. Adjusting for several important clinical and other risk factors, greater dietary plant protein intake was associated with reduced overall mortality in both sexes (hazard ratio per 1 SD was 0.95 [95% CI, 0.94-0.97] for men and 0.95 [95% CI, 0.93-0.96] for women; adjusted absolute risk difference per 1 SD was -0.36% [95% CI, -0.48% to -0.25%] for men and -0.33% [95% CI, -0.48% to -0.21%] for women; hazard ratio per 10 g/1000 kcal was 0.88 [95% CI, 0.84-0.91] for men and 0.86 [95% CI, 0.82-0.90] for women; adjusted absolute risk difference per 10 g/1000 kcal was -0.95% [95% CI, -1.3% to -0.68%] for men and -0.86% [95% CI, -1.3% to -0.55%] for women; all P < .001). The association between plant protein intake and overall mortality was similar across the subgroups of smoking status, diabetes, fruit consumption, vitamin supplement use, and self-reported health status. Replacement of 3% energy from animal protein with plant protein was inversely associated with overall mortality (risk decreased 10% in both men and women) and cardiovascular disease mortality (11% lower risk in men and 12% lower risk in women). In particular, the lower overall mortality was attributable primarily to substitution of plant protein for egg protein (24% lower risk in men and 21% lower risk in women) and red meat protein (13% lower risk in men and 15% lower risk in women).
Conclusions and relevance: In this large prospective cohort, higher plant protein intake was associated with small reductions in risk of overall and cardiovascular disease mortality. Our findings provide evidence that dietary modification in choice of protein sources may influence health and longevity.
Conflict of interest statement
Figures
Comment in
-
Protein Intake and Cause-Specific Mortality-Reply.JAMA Intern Med. 2021 Mar 1;181(3):407-408. doi: 10.1001/jamainternmed.2020.7260. JAMA Intern Med. 2021. PMID: 33346783 No abstract available.
-
Protein Intake and Cause-Specific Mortality.JAMA Intern Med. 2021 Mar 1;181(3):407-408. doi: 10.1001/jamainternmed.2020.7257. JAMA Intern Med. 2021. PMID: 33346813 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
