

Association of Delirium With Long-term Cognitive Decline: A Meta-analysis
- PMID: 32658246
- PMCID: PMC7358977
- DOI: 10.1001/jamaneurol.2020.2273
Association of Delirium With Long-term Cognitive Decline: A Meta-analysis
Erratum in
-
Error in Author Degrees and Reference List.JAMA Neurol. 2020 Nov 1;77(11):1452. doi: 10.1001/jamaneurol.2020.3284. JAMA Neurol. 2020. PMID: 32865555 Free PMC article. No abstract available.
Abstract
Importance: Delirium is associated with increased hospital costs, health care complications, and increased mortality. Long-term consequences of delirium on cognition have not been synthesized and quantified via meta-analysis.
Objective: To determine if an episode of delirium was an independent risk factor for long-term cognitive decline, and if it was, whether it was causative or an epiphenomenon in already compromised individuals.
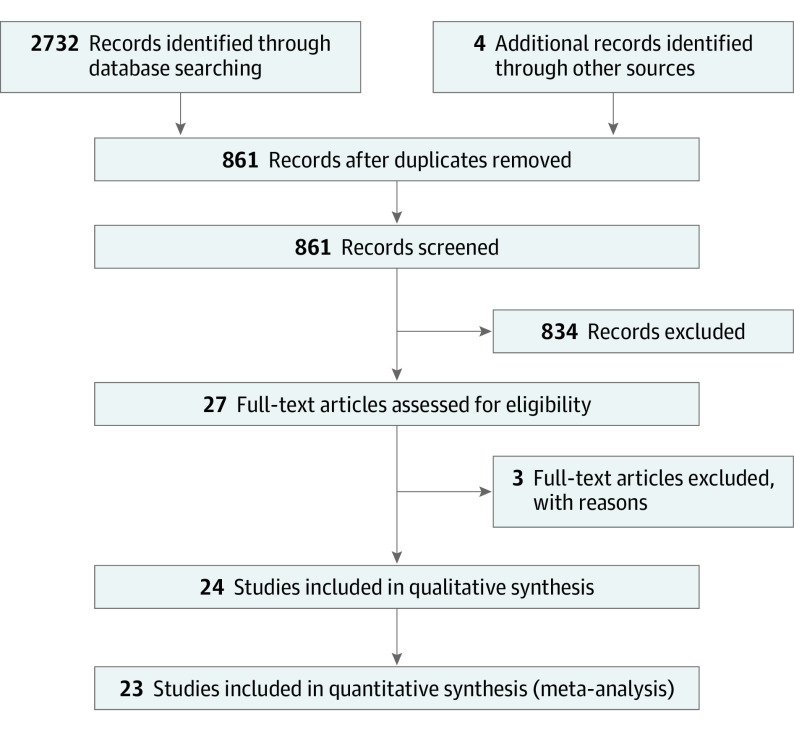
Data sources: A systematic search in PubMed, Cochrane, and Embase was conducted from January 1, 1965, to December 31, 2018. A systematic review guided by Preferred Reporting Items for Systematic Reviews and Meta-analyses was conducted. Search terms included delirium AND postoperative cognitive dysfunction; delirium and cognitive decline; delirium AND dementia; and delirium AND memory.
Study selection: Inclusion criteria for studies included contrast between groups with delirium and without delirium; an objective continuous or binary measure of cognitive outcome; a final time point of 3 or more months after the delirium episode. The electronic search was conducted according to established methodologies and was executed on October 17, 2018.
Data extraction and synthesis: Three authors extracted data on individual characteristics, study design, and outcome, followed by a second independent check on outcome measures. Effect sizes were calculated as Hedges g. If necessary, binary outcomes were also converted to g. Only a single effect size was calculated for each study.
Main outcomes and measures: The planned main outcome was magnitude of cognitive decline in Hedges g effect size in delirium groups when contrasted with groups that did not experience delirium.
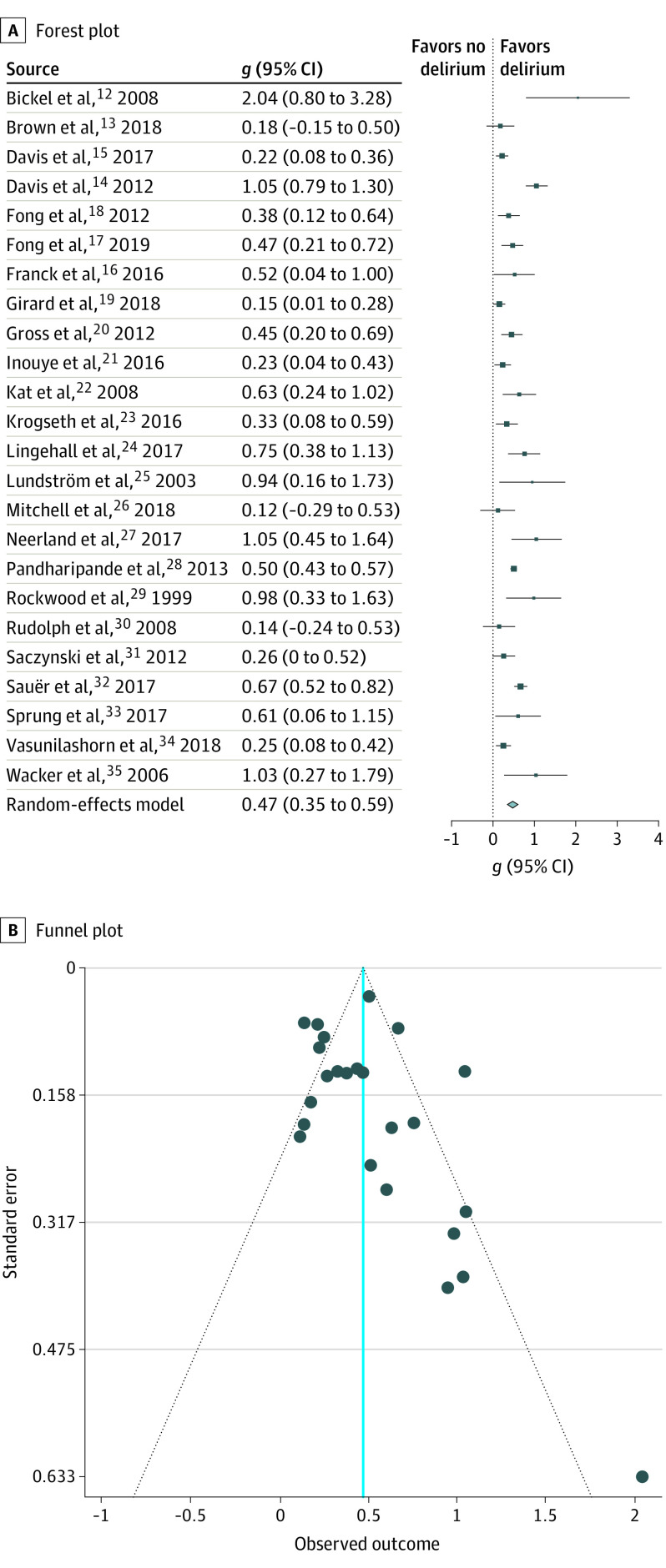
Results: Of 1583 articles, data subjected from the 24 studies (including 3562 patients who experienced delirium and 6987 controls who did not) were included in a random-effects meta-analysis for pooled effect estimates and random-effects meta-regressions to identify sources of study variance. One study was excluded as an outlier. There was a significant association between delirium and long-term cognitive decline, as the estimated effect size (Hedges g) for 23 studies was 0.45 (95% CI, 0.34-0.57; P < .001). In all studies, the group that experienced delirium had worse cognition at the final time point. The I2 measure of between-study variability in g was 0.81. A multivariable meta-regression suggested that duration of follow-up (longer with larger gs), number of covariates controlled (greater numbers were associated with smaller gs), and baseline cognitive matching (matching was associated with larger gs) were significant sources of variance. More specialized subgroup and meta-regressions were consistent with predictions that suggested that delirium may be a causative factor in cognitive decline.
Conclusions and relevance: In this meta-analysis, delirium was significantly associated with long-term cognitive decline in both surgical and nonsurgical patients.
Conflict of interest statement
Figures
Comment in
-
Delir erhöht Risiko kognitiver Defizite.MMW Fortschr Med. 2020 Dec;162(21-22):32. doi: 10.1007/s15006-020-4650-y. MMW Fortschr Med. 2020. PMID: 33319274 German. No abstract available.
References
-
- Inouye SK, Robinson T, Blaum C, et al. ; American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults . Postoperative delirium in older adults: best practice statement from the American Geriatrics Society. J Am Coll Surg. 2015;220(2):136-48.e1. doi: 10.1016/j.jamcollsurg.2014.10.019 - DOI - PubMed
