

SARS-CoV-2, COVID-19, skin and immunology - What do we know so far?
- PMID: 32658359
- PMCID: PMC7404682
- DOI: 10.1111/all.14498
SARS-CoV-2, COVID-19, skin and immunology - What do we know so far?
Abstract
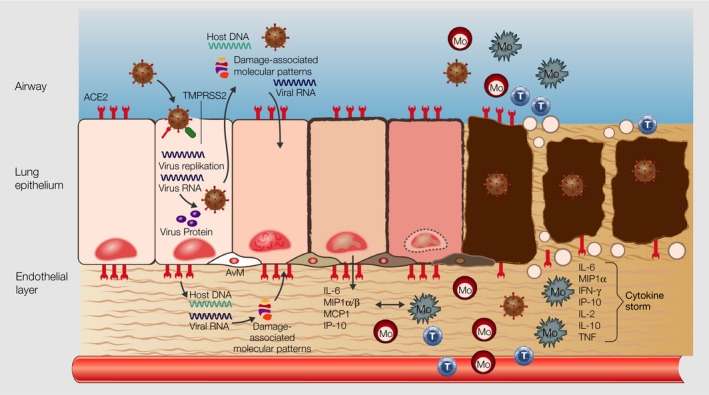
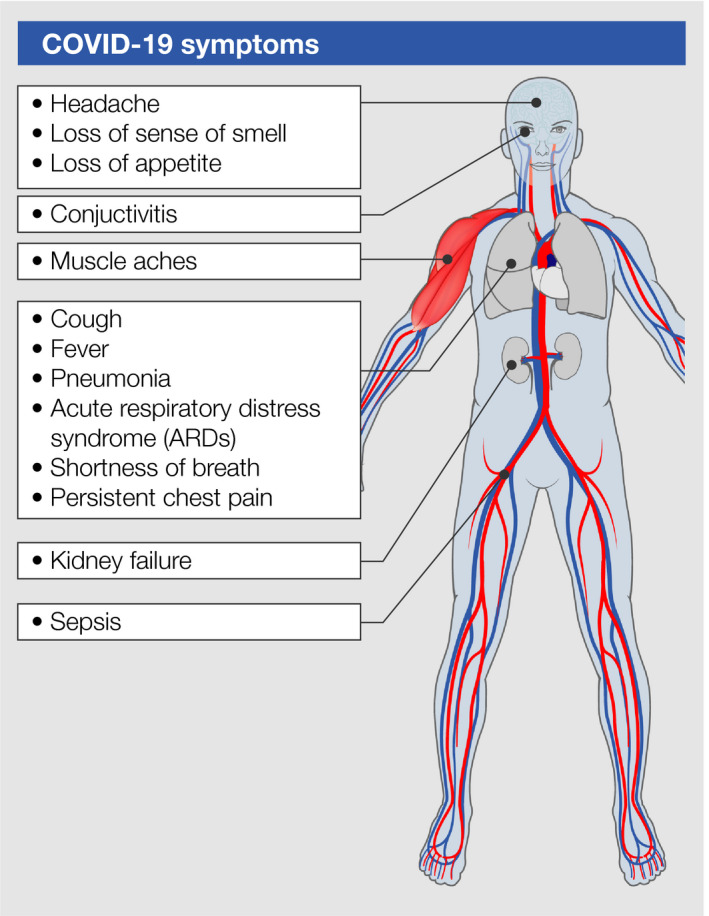
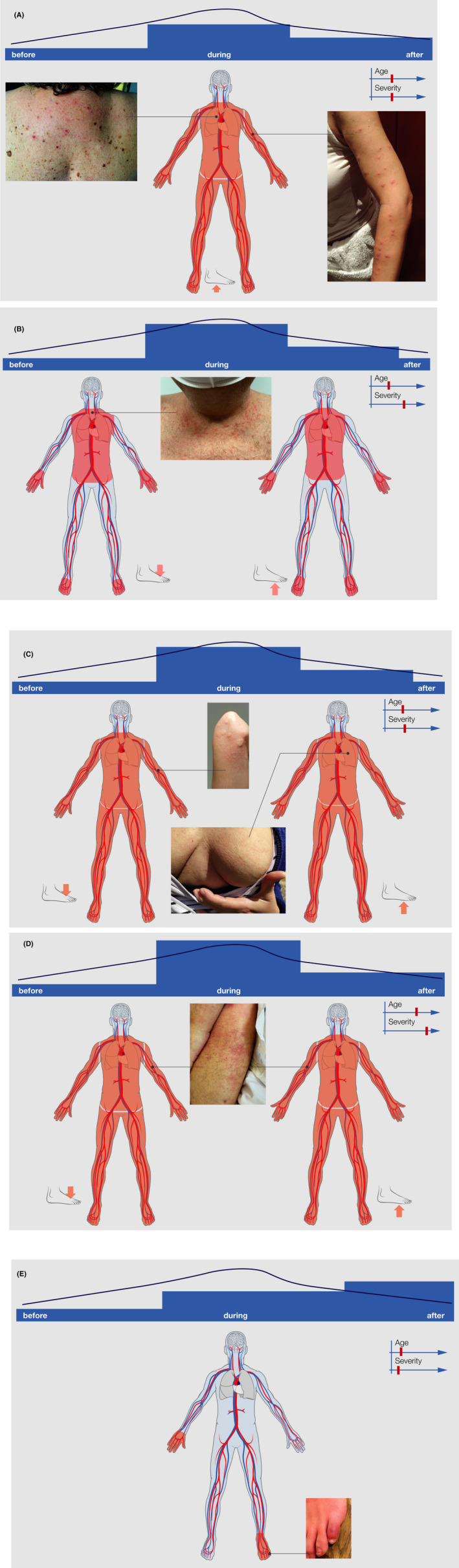
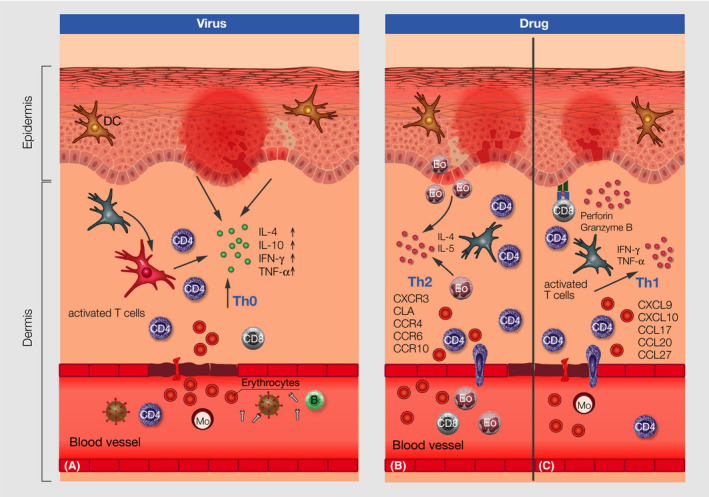
The pandemic condition coronavirus disease (COVID-19), caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), can take asymptomatic, mild, moderate, and severe courses. COVID-19 affects primarily the respiratory airways leading to dry cough, fever, myalgia, headache, fatigue, and diarrhea and can end up in interstitial pneumonia and severe respiratory failure. Reports about the manifestation of various skin lesions and lesions of the vascular system in some subgroups of SARS-CoV-2-positive patients as such features outside the respiratory sphere, are rapidly emerging. Vesicular, urticarial, and maculopapular eruptions and livedo, necrosis, and other vasculitis forms have been reported most frequently in association with SARS-CoV-2 infection. In order to update information gained, we provide a systematic overview of the skin lesions described in COVID-19 patients, discuss potential causative factors, and describe differential diagnostic evaluations. Moreover, we summarize current knowledge about immunologic, clinical, and histologic features of virus- and drug-induced lesions of the skin and changes to the vascular system in order to transfer this knowledge to potential mechanisms induced by SARS-CoV-2.
Keywords: allergy; drug hypersensitivity; skin; virus.
© 2020 The Authors. Allergy published by European Academy of Allergy and Clinical Immunology and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
