

A Model of Care Optimized for Marginalized Remote Population Unravels Migration Pattern in India
- PMID: 32659859
- PMCID: PMC7883670
- DOI: 10.1002/hep.31461
A Model of Care Optimized for Marginalized Remote Population Unravels Migration Pattern in India
Abstract
Background and aims: Access to basic health needs remains a challenge for most of world's population. In this study, we developed a care model for preventive and disease-specific health care for an extremely remote and marginalized population in Arunachal Pradesh, the northeasternmost state of India.
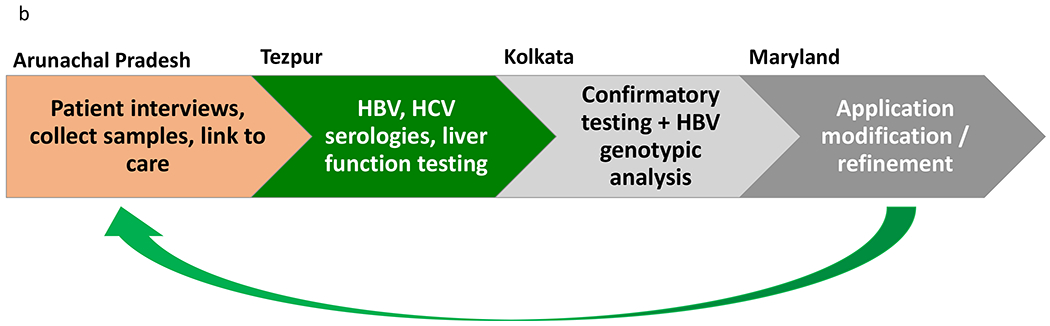
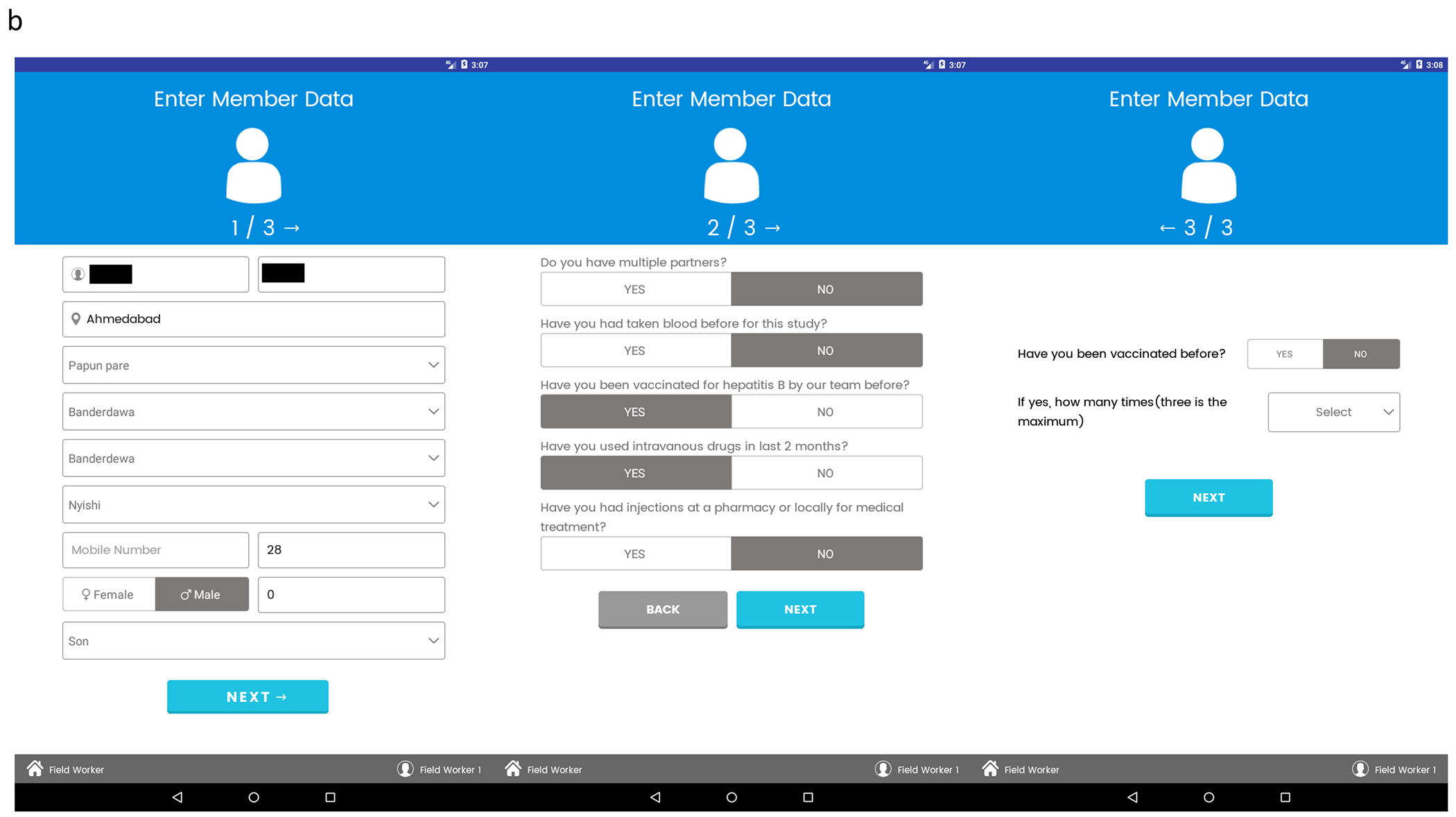
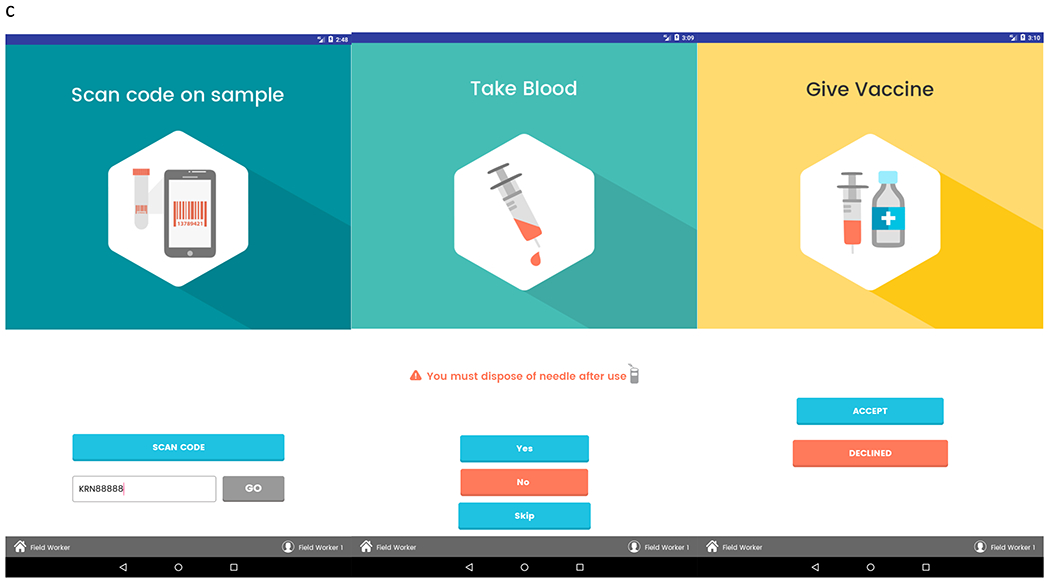
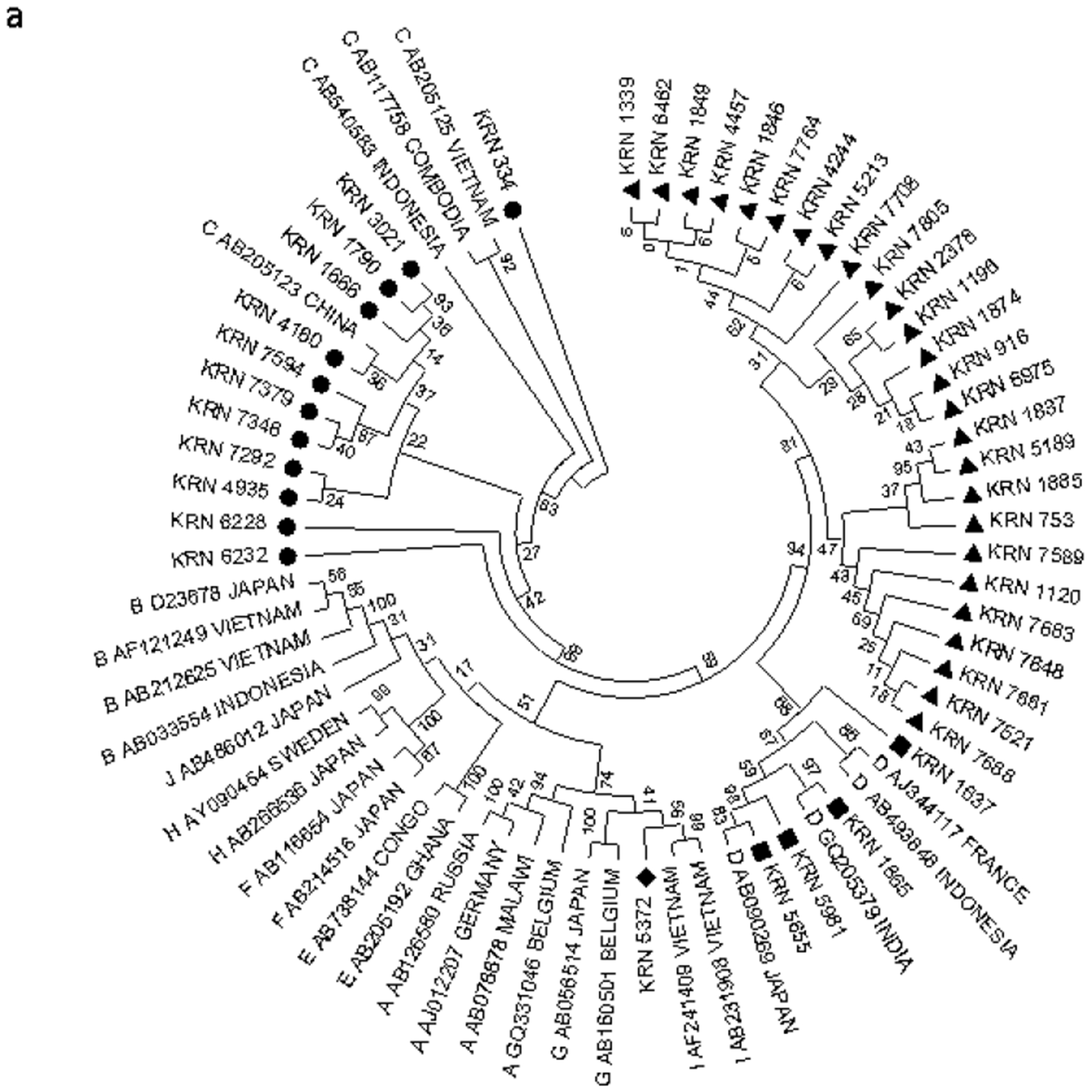
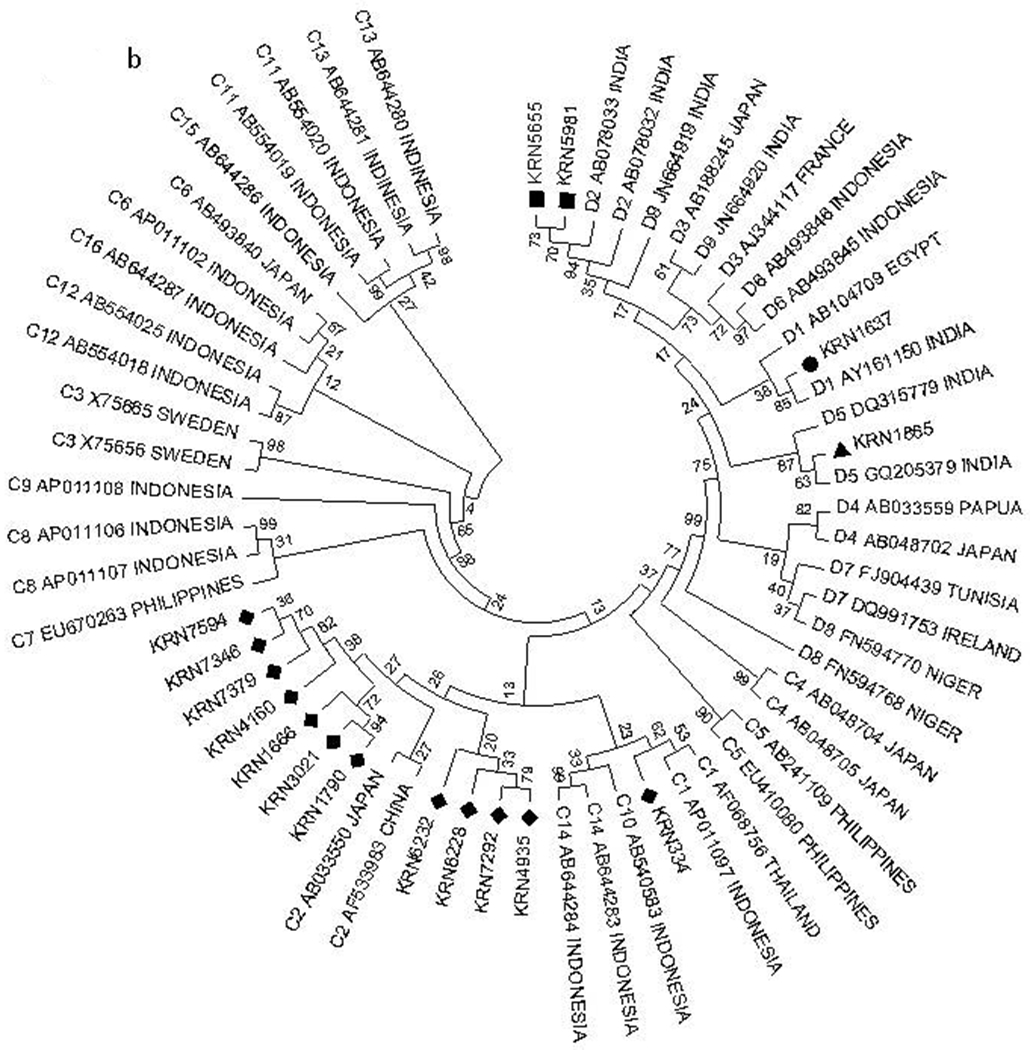
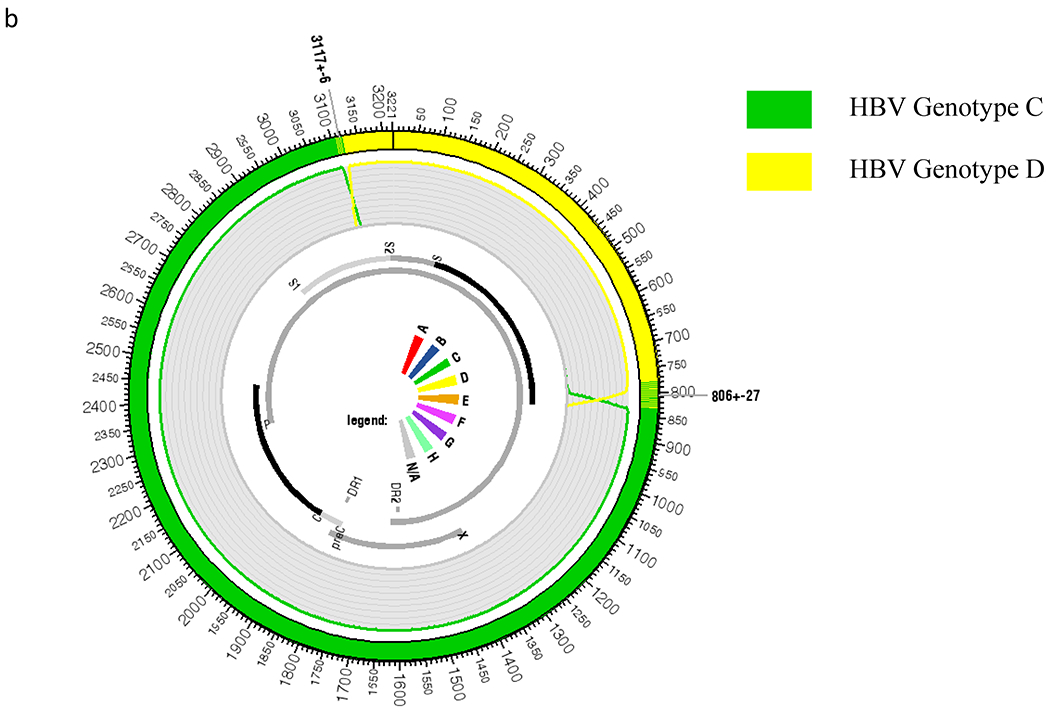
Approach and results: We performed patient screenings, performed interviews, and obtained blood samples in remote villages of Arunachal Pradesh through a tablet-based data collection application, which was later synced to a cloud database for storage. Positive cases of hepatitis B virus (HBV) were confirmed and genotyped in our central laboratory. The blood tests performed included liver function tests, HBV serologies, and HBV genotyping. HBV vaccination was provided as appropriate. A total of 11,818 participants were interviewed, 11,572 samples collected, and 5,176 participants vaccinated from the 5 westernmost districts in Arunachal Pradesh. The overall hepatitis B surface antigen (HBsAg) prevalence was found to be 3.6% (n = 419). In total, 34.6% were hepatitis B e antigen positive (n = 145) and 25.5% had HBV DNA levels greater than 20,000 IU/mL (n = 107). Genotypic analysis showed that many patients were infected with HBV C/D recombinants. Certain tribes showed high seroprevalence, with rates of 9.8% and 6.3% in the Miji and Nishi tribes, respectively. The prevalence of HBsAg in individuals who reported medical injections was 3.5%, lower than the overall prevalence of HBV.
Conclusions: Our unique, simplistic model of care was able to link a highly resource-limited population to screening, preventive vaccination, follow-up therapeutic care, and molecular epidemiology to define the migratory nature of the population and disease using an electronic platform. This model of care can be applied to other similar settings globally.
© 2020 by the American Association for the Study of Liver Diseases.
Figures




References
-
- Tang LSY, Covert E, Wilson E, Kottilil S. Chronic hepatitis B infection: a review. JAMA 2018;319:1802–1813. - PubMed
-
- World Health Organization. Combating hepatitis B and C to reach elimination by 2030. Geneva, Switzerland: World Health Organization; May 2016.
-
- Polaris Observatory Collaborators. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol 2018;3:383–403. - PubMed
-
- Scott N, Palmer A, Morgan C, Lesi O, Spearman CW, Sonderup M, et al. Cost-effectiveness of the controlled temperature chain for the hepatitis B virus birth dose vaccine in various global settings: a modelling study. Lancet Glob Health 2018;6:e659–e667. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
