

Choroidal origin of endogenous Candida endophthalmitis
- PMID: 32660583
- PMCID: PMC7359003
- DOI: 10.1186/s12886-020-01540-8
Choroidal origin of endogenous Candida endophthalmitis
Abstract
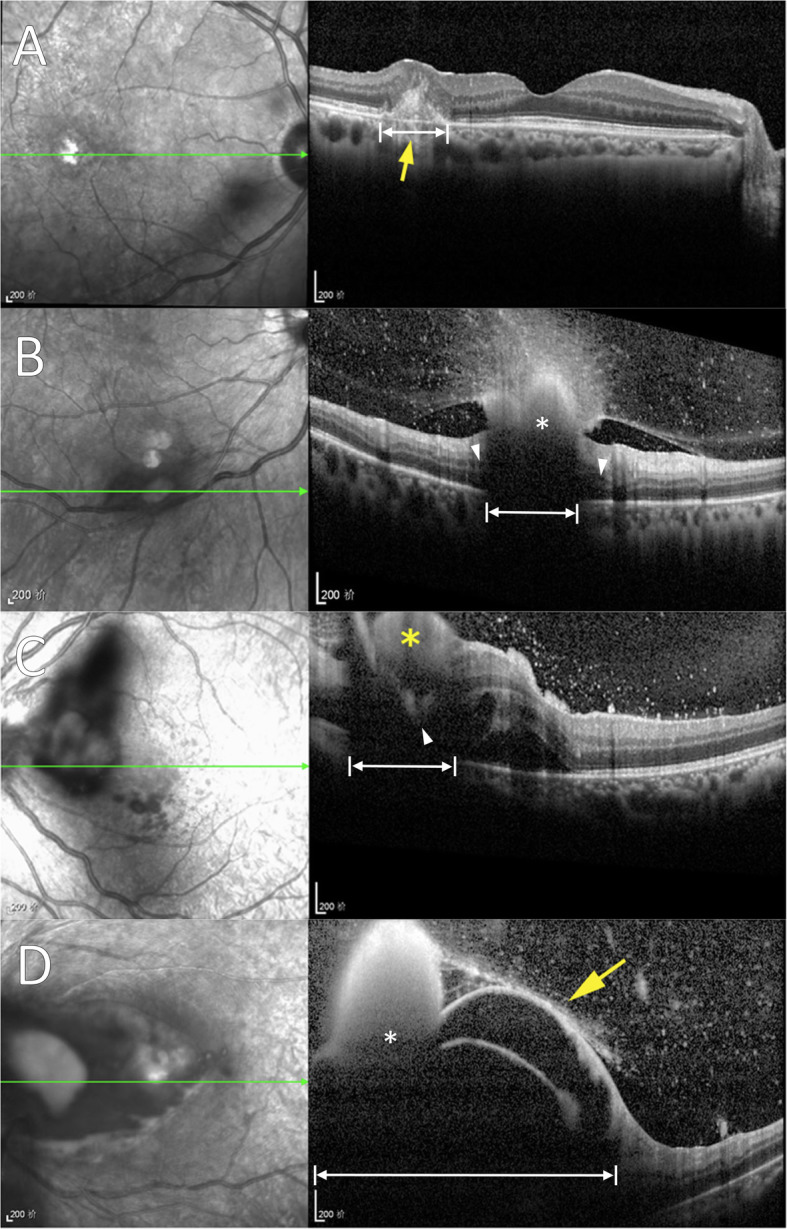
Endogenous Candida endophthalmitis (ECE) has been established with microscopic histopathology, both by autopsy and experimentation, to primarily originate from and involve the choroid. Zhuang et al. examined a series of patients with ECE using spectral-domain optical coherence tomography (SD-OCT) imaging and present a new classification scheme. The authors conclude the majority of lesions are primarily retinal in location without report of choroidal involvement. This discrepancy may be explained by posterior shadowing artifact and lack of discernment from associated retinal findings like infarction. These considerations are necessary in reviewing SD-OCT, characterizing ECE, and proposing new classification systems.
Keywords: Artifact; Choroid; Endogenous Candida endophthalmitis; Spectral-domain optical coherence tomography.
Conflict of interest statement
None.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
