

Intrathecal hydrophilic opioids for abdominal surgery: a meta-analysis, meta-regression, and trial sequential analysis
- PMID: 32660719
- PMCID: PMC7497029
- DOI: 10.1016/j.bja.2020.05.061
Intrathecal hydrophilic opioids for abdominal surgery: a meta-analysis, meta-regression, and trial sequential analysis
Abstract
Background: Intrathecal hydrophilic opioids decrease systemic opioid consumption after abdominal surgery and potentially facilitate enhanced recovery. A meta-analysis is needed to quantify associated risks and benefits.
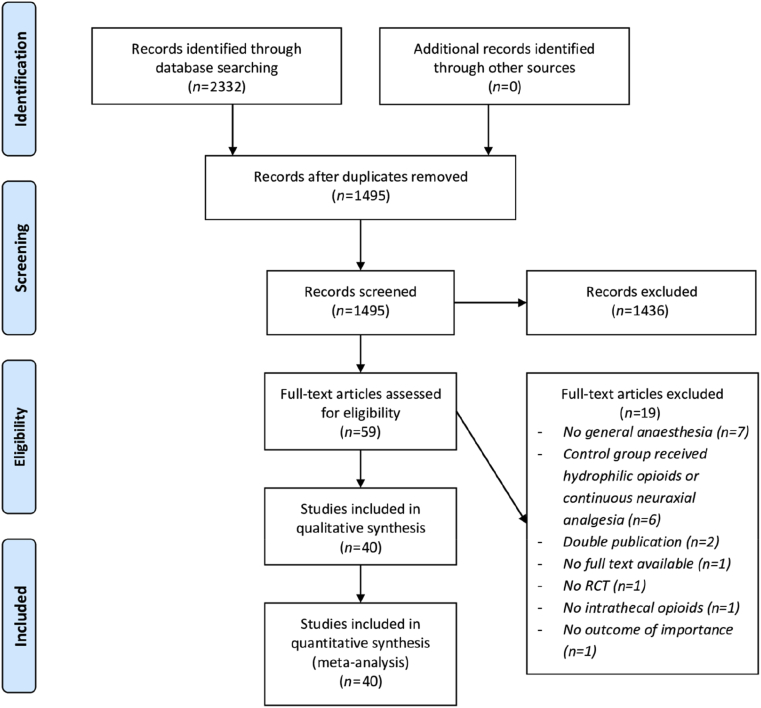
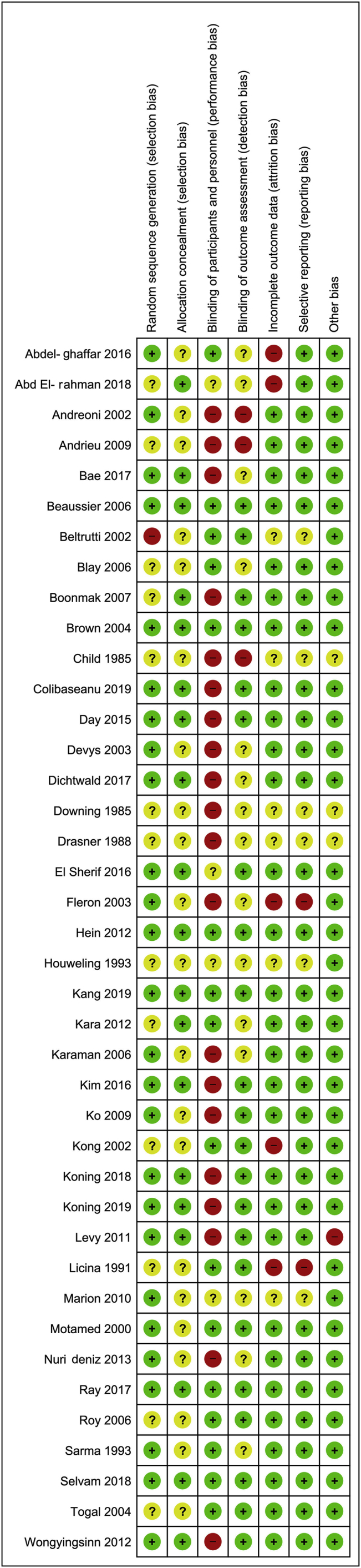
Methods: A systematic search was performed to find RCTs investigating intrathecal hydrophilic opioids in abdominal surgery. Caesarean section and continuous regional or neuraxial techniques were excluded. Several subgroup analyses were prespecified. A conventional meta-analysis, meta-regression, trial sequential analysis, and provision of GRADE scores were planned.
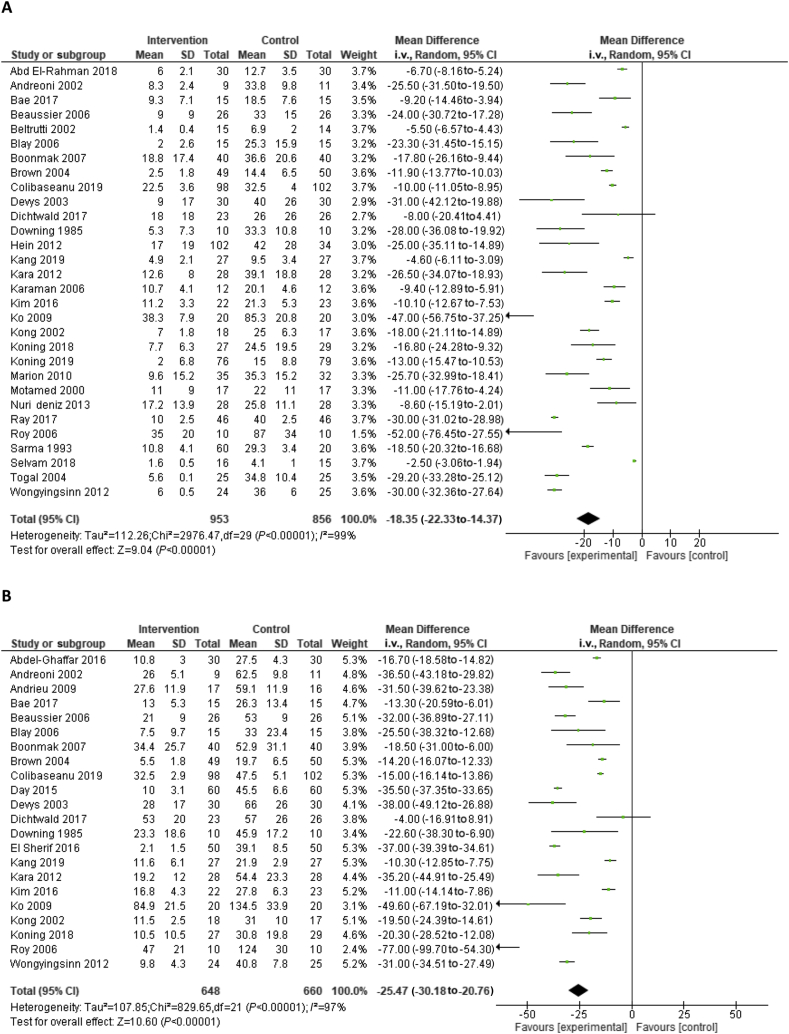
Results: The search yielded 40 trials consisting of 2500 patients. A difference was detected in 'i.v. morphine consumption' at Day 1 {mean difference [MD] -18.4 mg, (95% confidence interval [CI]: -22.3 to -14.4)} and Day 2 (MD -25.5 mg [95% CI: -30.2 to -20.8]), pain scores at Day 1 in rest (MD -0.9 [95% CI: -1.1 to -0.7]) and during movement (MD -1.2 [95% CI: -1.6 to -0.8]), length of stay (MD -0.2 days [95% CI: -0.4 to -0.1]) and pruritus (relative risk 4.3 [95% CI: 2.5-7.5]) but not in nausea or sedation. A difference was detected for respiratory depression (odds ratio 5.5 [95% CI: 2.1-14.2]) but not when two small outlying studies were excluded (odds ratio 1.4 [95% CI: 0.4-5.2]). The level of evidence was graded as high for morphine consumption, in part because the required information size was reached.
Conclusions: This study showed important opioid-sparing effects of intrathecal hydrophilic opioids. Our data suggest a dose-dependent relationship between the risk of respiratory depression and the dose of intrathecal opioids. Excluding two high-dose studies, intrathecal opioids have a comparable incidence of respiratory depression as the control group.
Clinical trial registration: PROSPERO-registry: CRD42018090682.
Keywords: analgesics; enhanced recovery; intrathecal; laparoscopy; laparotomy; opioids; spinal injections.
Copyright © 2020 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Gustafsson U.O., Scott M.J., Hubner M. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS(®)) society recommendations. World J Surg. 2018;43:659–695. - PubMed
-
- Wang J.K., Nauss L.A., Thomas J.E. Pain relief by intrathecally applied morphine in man. Anesthesiology. 1979;50:149–151. - PubMed
-
- Ummenhofer W.C., Arends R.H., Shen D.D., Bernards C.M. Comparative spinal distribution and clearance kinetics of intrathecally administered morphine, fentanyl, alfentanil, and sufentanil. Anesthesiology. 2000;92:739–753. - PubMed
-
- Levy B.F., Scott M.J., Fawcett W., Fry C. Randomized clinical trial of epidural, spinal or patient-controlled analgesia for patients undergoing laparoscopic colorectal surgery. Br J Surg. 2011;98:1068–1078. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
