

Prediction Model Based on the Combination of Cytokines and Lymphocyte Subsets for Prognosis of SARS-CoV-2 Infection
- PMID: 32661797
- PMCID: PMC7357264
- DOI: 10.1007/s10875-020-00821-7
Prediction Model Based on the Combination of Cytokines and Lymphocyte Subsets for Prognosis of SARS-CoV-2 Infection
Abstract
Background: There are currently rare satisfactory markers for predicting the death of patients with coronavirus disease 2019 (COVID-19). The aim of this study is to establish a model based on the combination of serum cytokines and lymphocyte subsets for predicting the prognosis of the disease.
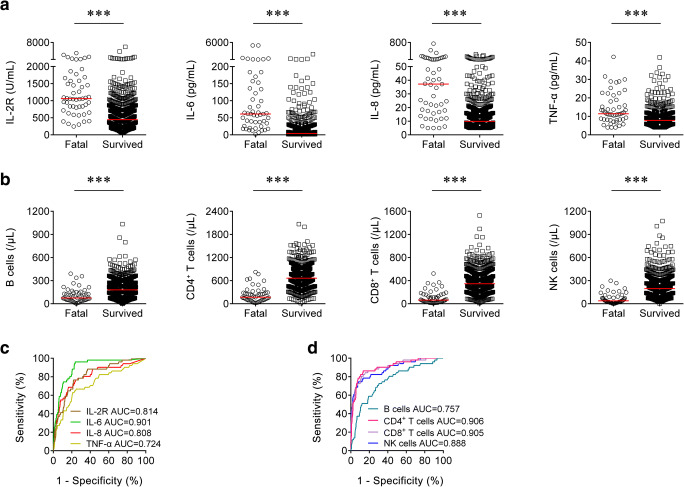
Methods: A total of 739 participants with COVID-19 were enrolled at Tongji Hospital from February to April 2020 and classified into fatal (n = 51) and survived (n = 688) groups according to the patient's outcome. Cytokine profile and lymphocyte subset analysis was performed simultaneously.
Results: The fatal patients exhibited a significant lower number of lymphocytes including B cells, CD4+ T cells, CD8+ T cells, and NK cells and remarkably higher concentrations of cytokines including interleukin-2 receptor, interleukin-6, interleukin-8, and tumor necrosis factor-α on admission compared with the survived subjects. A model based on the combination of interleukin-8 and the numbers of CD4+ T cells and NK cells showed a good performance in predicting the death of patients with COVID-19. When the threshold of 0.075 was used, the sensitivity and specificity of the prediction model were 90.20% and 90.26%, respectively. Meanwhile, interleukin-8 was found to have a potential value in predicting the length of hospital stay until death.
Conclusions: Significant increase of cytokines and decrease of lymphocyte subsets are found positively correlated with in-hospital death. A model based on the combination of three markers provides an attractive approach to predict the prognosis of COVID-19.
Keywords: Coronavirus disease 2019; cytokines; lymphocyte subsets; prognosis; severe acute respiratory syndrome coronavirus 2.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



References
-
- Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, Hu Y, Tao ZW, Tian JH, Pei YY, Yuan ML, Zhang YL, Dai FH, Liu Y, Wang QM, Zheng JJ, Xu L, Holmes EC, Zhang YZ. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579:265–269. doi: 10.1038/s41586-020-2008-3. - DOI - PMC - PubMed
-
- World Health Organization, Novel coronavirus (2019-ncov) situation report 103. Available online:https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio... (accessed on 3 May 2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
